

Sodium-Glucose Co-Transporter 2 Inhibitors for Non-Alcoholic Fatty Liver Disease in Asian Patients With Type 2 Diabetes: A Meta-Analysis
- PMID: 33643221
- PMCID: PMC7905212
- DOI: 10.3389/fendo.2020.609135
Sodium-Glucose Co-Transporter 2 Inhibitors for Non-Alcoholic Fatty Liver Disease in Asian Patients With Type 2 Diabetes: A Meta-Analysis
Abstract
Objective: Non-alcoholic fatty liver disease (NAFLD) is a very common disorder among patients with type 2 diabetes and may share causal relationship. Type 2 diabetes is a risk factor for progression and potential poor outcomes in NAFLD patients. This meta-analysis aimed to analyze the current evidence of sodium-glucose co-transporter-2 inhibitors (SGLT2i), a glucose-lowering drug to improve NAFLD in patients with Type 2 Diabetes.
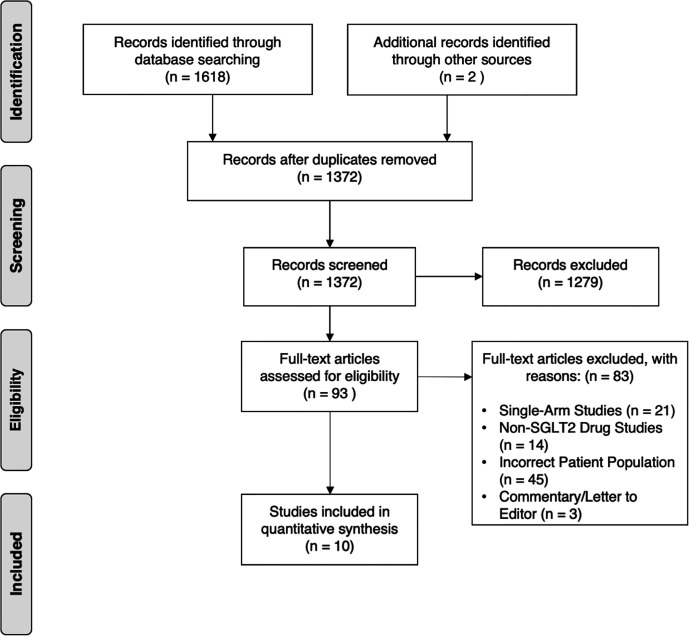
Methods: Medline, Embase and Cochrane Central Register of Controlled Trials were searched for articles examining efficacy of SGLT2i on treatments of NAFLD in type 2 diabetes in July 2020, and articles were sieved. Continuous data were extracted in the form of mean and standard deviation and were pooled with standardized mean difference (SMD).
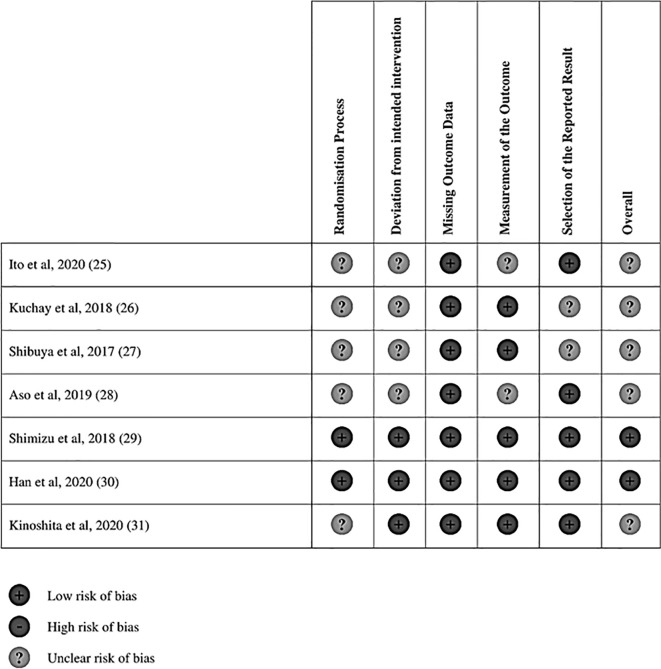
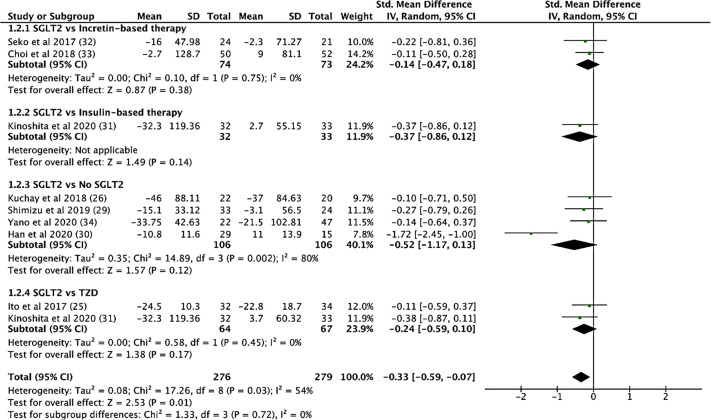
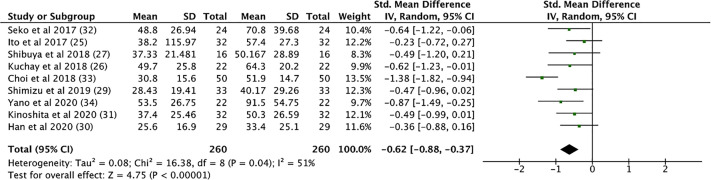
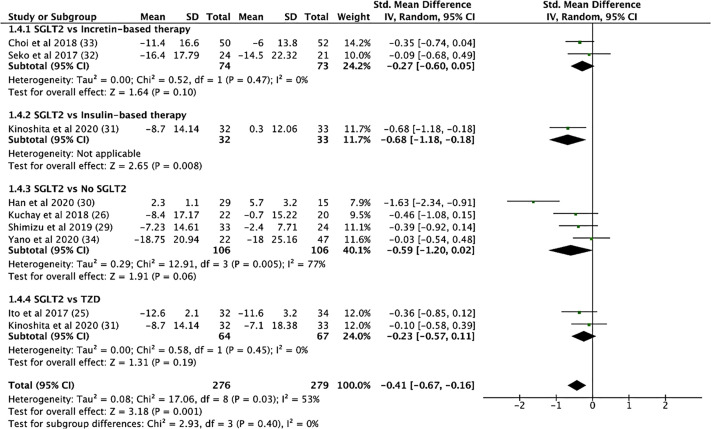
Results: 10 articles involving 555 patients from seven randomized controlled trials (RCTs) and three cohort studies, were included in this meta-analysis. Our analysis revealed significant improvements in hepatic fat content (after treatment: -0.789 (-1.404 to -0.175), p = 0.012; compared with control: -0.923 (-1.562 to -0.285), p = 0.005), AST (After Treatment: -0.539 (-0.720 to -0.357), p < 0.001; compared with control: -0.421 (-0.680 to -0.161), p = 0.001), ALT (after treatment: -0.633 (-0.892 to -0.373), p < 0.001; compared with Control: -0.468 (-0.685 to -0.251), p < 0.001), body composition (BMI: after treatment: -0.225 (-0.456 to 0.005), p = 0.055; compared with Control: -1.092 (-2.032 to -0.153), p = 0.023), glycemic control (HbA1c: After Treatment: -0.701 (-1.098 to -0.303), p = 0.001; compared with control: -0.210 (-0.603 to 0.183), p = 0.295), lipid parameters (Triglycerides: after treatment: -0.230 (-0.409 to -0.052), p = 0.011; compared with control: -0.336 (-0.597 to -0.076), p = 0.011), inflammatory markers (serum ferritin: after treatment: -0.409 (-0.694 to -0.124), p = 0.005; compared with control: -0.814 (-1.688 to 0.059), p = 0.068) after SGLT2i treatment, and when compared against controls. There was a trend in the improvement in fibrosis markers after SGLT2i treatment.
Conclusions: SGLT2i is an effective treatment to improve NAFLD among patients with type 2 diabetes. Further studies are needed to understand the direct and indirect effects of SGLT2i on NAFLD and if SGLT2i could prevent the progression of NAFLD or NASH. SGLT2i could potentially be considered for patients with type 2 diabetes and NAFLD, if there are no contraindications.
Keywords: hepatic fat; meta-analysis; non-alcoholic fatty liver disease; sodium-glucose co-transporter-2 inhibitors; type 2 diabetes.
Copyright © 2021 Wong, Yaow, Ng, Chin, Low, Lim, Muthiah and Khoo.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The reviewer KV declared a shared affiliation with the authors to the handling editor at time of review.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical