

The effect of timing of initiation of renal replacement therapy on mortality: A retrospective case-control study
- PMID: 33643427
- PMCID: PMC7890751
- DOI: 10.1177/1751143719892792
The effect of timing of initiation of renal replacement therapy on mortality: A retrospective case-control study
Abstract
Purpose: To determine if earlier initiation of renal replacement therapy (RRT) is associated with improved survival in patients with severe acute kidney injury.
Methods: We performed a retrospective case-control study of propensity-matched groups with multivariable logistic regression using Akaike Information Criteria to adjust for non-matched variables in a surgical ICU in a tertiary care hospital.
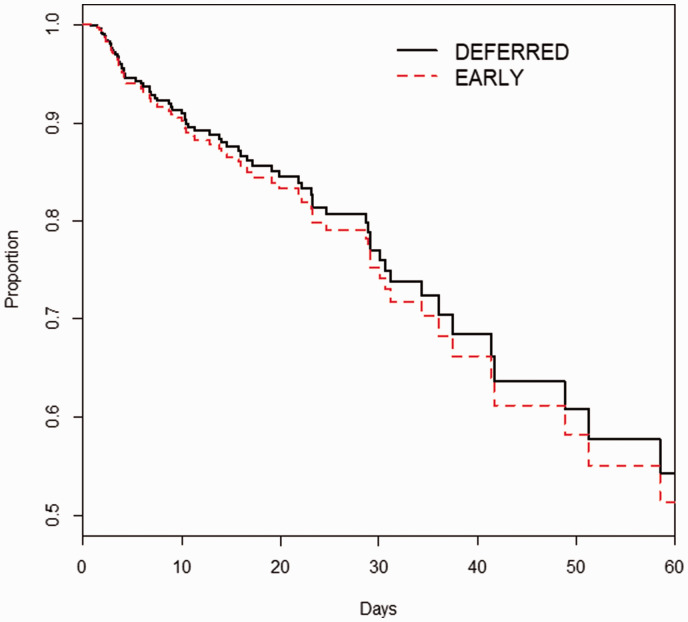
Results: We matched 169 of 205 (82%) patients with new initiation of RRT (EARLY group) to 169 similar patients who did not initiate RRT on that day (DEFERRED group). Eighteen (11%) of DEFERRED eventually received RRT before discharge. By univariate analysis, ICU mortality was higher in EARLY (n = 60 (36%) vs. n = 23 (14%), p < 0.001) as was hospital mortality (n = 73 (43%) vs. n = 44 (26%), p = 0.001). Of the 18 RRT patients in DEFERRED, 12 (67%) died in ICU and 13 (72%) in hospital. After propensity matching and logistic regression, we found that EARLY initiation of RRT was associated with a more than doubling of ICU mortality (aOR = 2.310, 95% confidence interval = 1.254-4.257, p = 0.007). However, after similar adjustment, there was no difference in hospital mortality (aOR = 1.283, 95% CI = 0.753-2.186, p = 0.360).
Conclusions: While ICU mortality was increased in the EARLY group, there was no difference in hospital mortality between EARLY and DEFERRED groups.
Keywords: Acute kidney injury; creatinine; propensity matching; renal replacement therapy.
© The Intensive Care Society 2019.
Conflict of interest statement
Declaration of conflicting interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures


References
-
- Bagshaw SM, George C, Bellomo R, et al. A comparison of the RIFLE and AKIN criteria for acute kidney injury in critically ill patients. Nephrol Dial Transplant 2008; 23: 1569–1574. - PubMed
-
- Wald R, McArthur E, Adhikari NK, et al. Changing incidence and outcomes following dialysis-requiring acute kidney injury among critically ill adults: a population-based cohort study. Am J Kidney Dis 2015; 65: 870–877. - PubMed
-
- Hoste EA, Schurgers M. Epidemiology of acute kidney injury: how big is the problem? Crit Care Med 2008; 36: S146–S151. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources