

Combined High-Dose LATTICE Radiation Therapy and Immune Checkpoint Blockade for Advanced Bulky Tumors: The Concept and a Case Report
- PMID: 33643893
- PMCID: PMC7907519
- DOI: 10.3389/fonc.2020.548132
Combined High-Dose LATTICE Radiation Therapy and Immune Checkpoint Blockade for Advanced Bulky Tumors: The Concept and a Case Report
Abstract
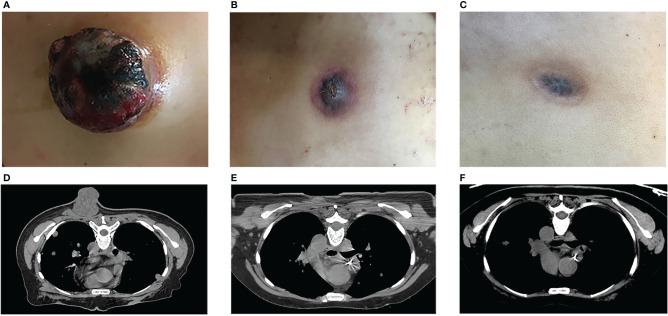
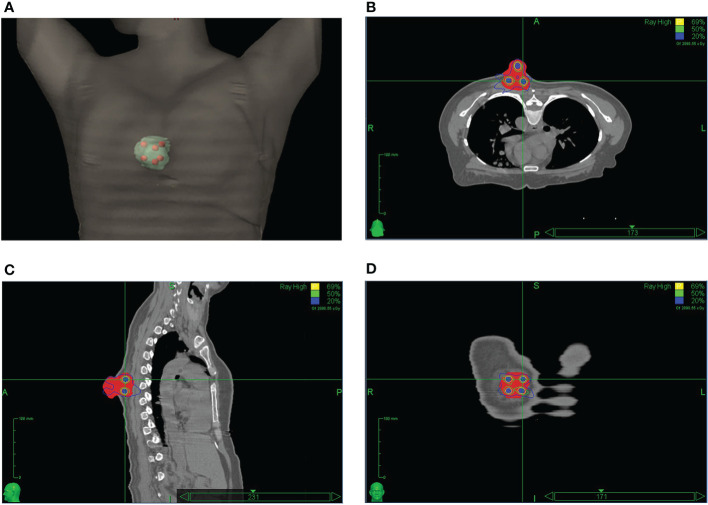
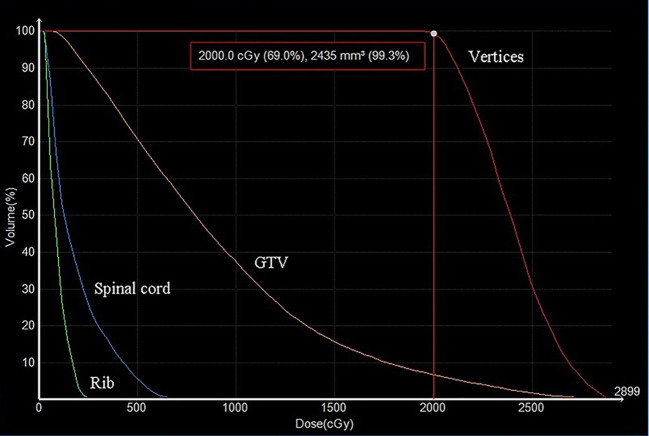
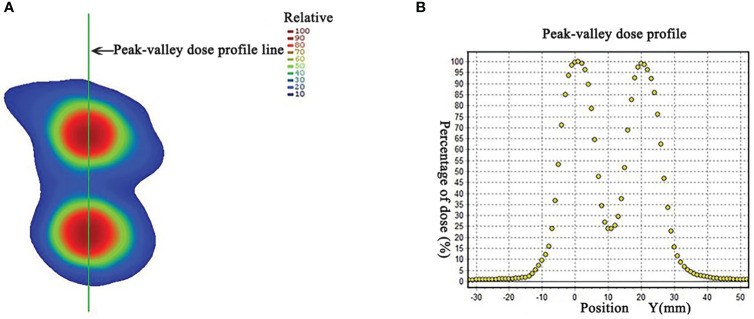
Although the combination of immune checkpoint blockades with high dose of radiation has indicated the potential of co-stimulatory effects, consistent clinical outcome has been yet to be demonstrated. Bulky tumors present challenges for radiation treatment to achieve high rate of tumor control due to large tumor sizes and normal tissue toxicities. As an alternative, spatially fractionated radiotherapy (SFRT) technique has been applied, in the forms of GRID or LATTICE radiation therapy (LRT), to safely treat bulky tumors. When used alone in a single or a few fractions, GRID or LRT can be best classified as palliative or tumor de-bulking treatments. Since only a small fraction of the tumor volume receive high dose in a SFRT treatment, even with the anticipated bystander effects, total tumor eradications are rare. Backed by the evidence of immune activation of high dose radiation, it is logical to postulate that the combination of High-Dose LATTICE radiation therapy (HDLRT) with immune checkpoint blockade would be effective and could subsequently lead to improved local tumor control without added toxicities, through augmenting the effects of radiation in-situ vaccine and T-cell priming. We herein present a case of non-small cell lung cancer (NSCLC) with multiple metastases. The patient received various types of palliative radiation treatments with combined chemotherapies and immunotherapies to multiple lesions. One of the metastatic lesions measuring 63.2 cc was treated with HDLRT combined with anti-PD1 immunotherapy. The metastatic mass regressed 77.84% over one month after the treatment, and had a complete local response (CR) five months after the treatment. No treatment-related side effects were observed during the follow-up exams. None of the other lesions receiving palliative treatments achieved CR. The dramatic differential outcome of this case lends support to the aforementioned postulate and prompts for further systemic clinical studies.
Keywords: bulky tumor; high-dose LATTICE radiation therapy; immunotherapy; lattice radiotherapy; non-small cell lung cancer; spatially fractionated radiotherapy.
Copyright © 2021 Jiang, Li, Zhang, Li, Dong, Chen, Lin, Zhang, Zheng, Yan, Zheng, Wu and Xu.
Conflict of interest statement
YZ and XW were employed by Executive Medical Physics Associates. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Trifiletti D, Chao S, Sahgal A, Sheehan J. eds. Stereotactic Radiosurgery and Stereotactic Body Radiation Therapy. Cham: Springer; (2019). 10.1007/978-3-030-16924-4 - DOI
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials