

Strain Distribution and Drug Susceptibility of Invasive Fungal Infection in Clinical Patients With Systemic Internal Diseases
- PMID: 33644009
- PMCID: PMC7906281
- DOI: 10.3389/fbioe.2020.625024
Strain Distribution and Drug Susceptibility of Invasive Fungal Infection in Clinical Patients With Systemic Internal Diseases
Abstract
Background: Patients with systemic internal diseases present high risks for invasive fungal infections, which results in increased morbidity and mortality. Identification of high-risk departments and susceptibility systems could help to reduce the infective rate clinically. Correct selection of sensitive anti-fungal drugs not only could improve the cure rate but also could reduce the adverse reactions and complications caused by long-term antifungal drug treatment, which can be especially important in patients with serious systemic diseases. Therefore, the distribution changes of invasive fungal strains in patients with systemic internal diseases and the choice of antifungal drugs in clinical practice should be updated.
Objective: This work aimed to investigate the incidence, strain distributions, and drug susceptibility of invasive fungal strains isolated from patients with systemic internal diseases.
Methods: Samples were collected from 9,430 patients who were diagnosed with internal diseases in our hospital from January to December 2018. We then cultured and identified the fungal strains using API 20C AUX. We performed drug sensitivity analysis via the ATB Fungus-3 fungal susceptibility strip. Resistance was defined using the revised Clinical Laboratory Standardization Committee of United States breakpoints/epidemiological cutoff values to assign susceptibility or wild-type status to systemic antifungal agents.
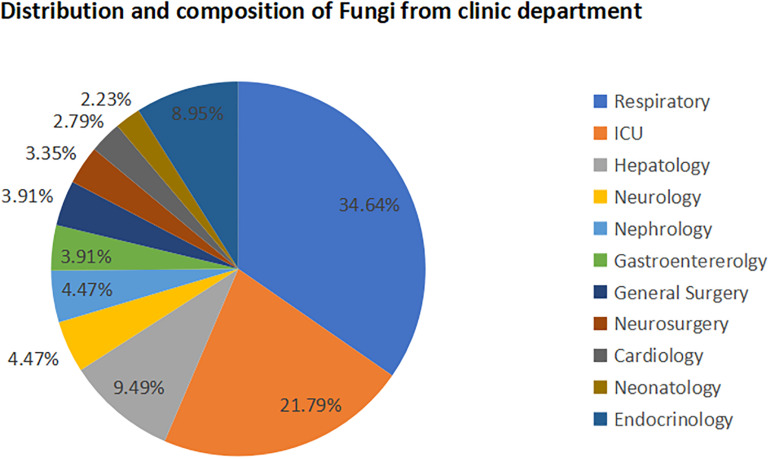
Results: A total of 179 patients (49 female, 130 male) with fungal infection were included. The high-incidence departments were determined to be the respiratory department (34.64%), intensive care unit (ICU; 21.79%), and hepatology department (9.50%). The susceptible systems for infection were the respiratory tract (sputum, 68.72%, 123/179; secretion retained in the tracheal catheter, 3.35%, 6/179), urinary tract (urine, 9.50%, 17/179), and gastrointestinal tract (feces, 9.50%, 17/179). The major pathogens were Candida (90.50%), Aspergillus (8.93%), and Cryptococcus neoformans (0.56%). The infective candida subgroups were Candida albicans (70.95%), Candida krusei (6.15%), Candida glabrata (5.59%), Candida parapsilosis (3.91%), and Candida tropicalis (3.91%). The susceptibility of non-Aspergillus fungi for amphotericin B was 100.0%. The susceptibility rates of 5-fluorocytocine (5-FC) and voriconazole were 72.73 and 81.82%, respectively, for C. krusei, 98.43 and 100% for C. albicans, and 100% for both drugs for C. glabrata, C. parapsilosis, and C. tropicalis. The susceptibility rates of fluconazole and itraconazole were 0 and 54.55%, respectively, for C. krusei, 20 and 20% for C. glabrata, and 57.14 and 57.14% for C. tropicalis. The resistance rate of C. tropicalis for both fluconazole and itraconazole was 41.43%.
Conclusion: Patients in the respiratory department, ICU, and hepatology department presented high rates of invasive fungal infections and should include special attention during clinical treatment. The respiratory tract, urinary tract, and gastrointestinal tract were the susceptible systems. Candida, especially C. albicans, was the main pathogen. From the perspective of drug sensitivity, amphotericin B should be given priority in treating the non-Aspergillus fungi infection in patients with systemic internal diseases, while the susceptibility of invasive fungal strains to azoles was variant. These data might provide clinical evidence for the prevention and treatment of invasive fungal infection in patients with systemic internal diseases.
Keywords: drug resistance; drug susceptibility; epidemiology; invasive fungal infection; systemic internal diseases.
Copyright © 2021 Zeng, Peng, Liu, Huang, Zhang, Wen, Lai and Zheng.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Candida and candidaemia. Susceptibility and epidemiology.Dan Med J. 2013 Nov;60(11):B4698. Dan Med J. 2013. PMID: 24192246 Review.
-
[Antifungal susceptibility profiles of Candida species to triazole: application of new CLSI species-specific clinical breakpoints and epidemiological cutoff values for characterization of antifungal resistance].Mikrobiyol Bul. 2016 Jan;50(1):122-32. doi: 10.5578/mb.10682. Mikrobiyol Bul. 2016. PMID: 27058336 Turkish.
-
Antifungal susceptibilities of Candida glabrata species complex, Candida krusei, Candida parapsilosis species complex and Candida tropicalis causing invasive candidiasis in China: 3 year national surveillance.J Antimicrob Chemother. 2015 Mar;70(3):802-10. doi: 10.1093/jac/dku460. Epub 2014 Dec 3. J Antimicrob Chemother. 2015. PMID: 25473027
-
Candida species distribution and antifungal susceptibility testing according to European Committee on Antimicrobial Susceptibility Testing and new vs. old Clinical and Laboratory Standards Institute clinical breakpoints: a 6-year prospective candidaemia survey from the fungal infection network of Switzerland.Clin Microbiol Infect. 2014 Jul;20(7):698-705. doi: 10.1111/1469-0691.12440. Epub 2013 Dec 12. Clin Microbiol Infect. 2014. PMID: 24188136
-
Resistance in human pathogenic yeasts and filamentous fungi: prevalence, underlying molecular mechanisms and link to the use of antifungals in humans and the environment.Dan Med J. 2016 Oct;63(10):B5288. Dan Med J. 2016. PMID: 27697142 Review.
Cited by
-
Macrophage polarization-related gene SOAT1 is involved in inflammatory response and functional recovery after spinal cord injury.Mol Cell Biochem. 2025 Jul;480(7):4197-4212. doi: 10.1007/s11010-025-05246-7. Epub 2025 Mar 6. Mol Cell Biochem. 2025. PMID: 40050510
-
Epidemiology, Drug Susceptibility, and Clinical Risk Factors in Patients With Invasive Aspergillosis.Front Public Health. 2022 Apr 15;10:835092. doi: 10.3389/fpubh.2022.835092. eCollection 2022. Front Public Health. 2022. PMID: 35493371 Free PMC article.
-
Deep Fungal Infections Among General Hospital Inpatients in Southwestern China: A 5-Year Retrospective Study.Front Public Health. 2022 Mar 28;10:842434. doi: 10.3389/fpubh.2022.842434. eCollection 2022. Front Public Health. 2022. PMID: 35419337 Free PMC article.
-
Multilocus Sequence Typing and Antifungal Susceptibility of Vaginal and Non-vaginal Candida glabrata Isolates From China.Front Microbiol. 2022 Mar 17;13:808890. doi: 10.3389/fmicb.2022.808890. eCollection 2022. Front Microbiol. 2022. PMID: 35369470 Free PMC article.
-
Distribution and antifungal susceptibility pattern of Candida species from mainland China: A systematic analysis.Virulence. 2022 Dec;13(1):1573-1589. doi: 10.1080/21505594.2022.2123325. Virulence. 2022. PMID: 36120738 Free PMC article. Review.
References
-
- Anaissie E. J., McGinnis M. R., Pfaller M. A. (2009). Clinical Mycology. Amsterdam: Elsevier Health Science.
-
- Bloos F., Bayer O., Sachse S., Straube E., Reinhart K., Kortgen A. J. J. O. C. C. (2013). Attributable costs of patients with candidemia and potential implications of polymerase chain reaction–based pathogen detection on antifungal therapy in patients with sepsis. J. Crit. Care 28 2–8. 10.1016/j.jcrc.2012.07.011 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources