

A Cost-Utility Analysis of Switching from Reference to Biosimilar Infliximab Compared to Maintaining Reference Infliximab in Adult Patients with Crohn's Disease
- PMID: 33644677
- PMCID: PMC7898373
- DOI: 10.1093/jcag/gwz045
A Cost-Utility Analysis of Switching from Reference to Biosimilar Infliximab Compared to Maintaining Reference Infliximab in Adult Patients with Crohn's Disease
Erratum in
-
Erratum.J Can Assoc Gastroenterol. 2020 Mar 19;4(1):50. doi: 10.1093/jcag/gwaa008. eCollection 2021 Feb. J Can Assoc Gastroenterol. 2020. PMID: 34164604 Free PMC article.
Abstract
Background and aims: Lower-cost biosimilar infliximab may address affordability concerns in the treatment of adults with Crohn's disease (CD), however, evidence regarding the cost-effectiveness of switching from reference to biosimilar is warranted. The aim of this research was to assess the incremental cost of switching from treatment with reference infliximab to biosimilar compared with maintaining reference infliximab in adults with CD per quality-adjusted life year (QALY) gained.
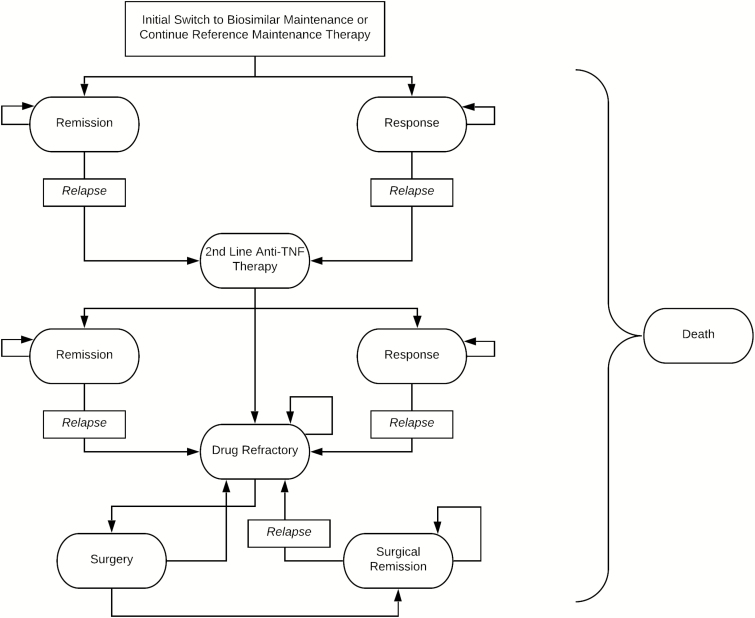
Methods: A probabilistic cohort Markov model with 8-week cycle lengths was constructed to estimate the incremental costs and effects of switching over a 5-year time horizon from a public payer perspective. Base-case clinical inputs were obtained from NOR-SWITCH subgroup analyses and other published trials. Costs were obtained from Canadian sources. A total of 10,000 simulations were run. Sensitivity analysis was used to test the robustness of the results to variations in uncertain parameters.
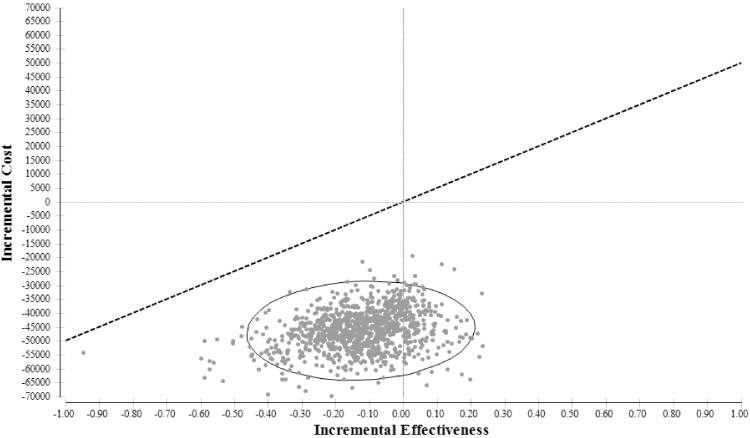
Results: Switching to biosimilar infliximab was less costly but also less effective with incremental savings of $46,194 (95% confidence interval [CI]: $42,420, $50,455) and a loss in QALYs of -0.13 (95% CI: -0.16, -0.07). Eighty-three per cent of the simulations demonstrated incremental cost savings and an incremental loss of effectiveness. The model was sensitive to differences in rates of disease worsening between reference and biosimilar infliximab.
Conclusions: While biosimilar infliximab is associated with incremental savings for patients on maintenance therapy who are switched from reference infliximab, funding decision makers must decide whether a small loss of effectiveness is justified. Further evidence will help to inform reimbursement policy.
Keywords: Cost-utility analysis; Crohn’s disease; Infliximab.
© The Author(s) 2020. Published by Oxford University Press on behalf of the Canadian Association of Gastroenterology.
Figures
References
-
- Lybecker KM. The Biologics Revolution in the Production of Drugs. Fraser Institute, July 2016. <https://www.fraserinstitute.org/sites/default/files/biologics-revolution...> (Accessed July 2017).
-
- National Prescription Drug Utilization Information System. Potential Savings from Biosimilars in Canada. <http://www.pmprb-cepmb.gc.ca/view.asp?ccid=1304> (Accessed February 2018).
-
- IMS Brogan. IMS Brogan Private Drug Plan Drug Cost Forecast Commissioned by Rx&D. November, 2013. <http://innovativemedicines.ca/wp-content/uploads/2015/05/20131125_Report...> (Accessed July 2017).
-
- Canadian Institute for Health Information. Prescribed Drug Spending in Canada, 2017, Ottawa, Ontario: A Focus on Public Drug Programs, 2017. <https://secure.cihi.ca/free_products/pdex2017-report-en.pdf> (Accessed July 2017).
-
- IQVIA Institute for Human Data Science. Advancing Biosimilar Sustainability in Europe: A Multi-Stakeholder Assessment. Parsippany, NJ: IQVIA Institute for Human Data Science, September 4, 2018.
LinkOut - more resources
Full Text Sources