

Identifying key factors for the effectiveness of pancreatic cancer screening: A model-based analysis
- PMID: 33644856
- PMCID: PMC8251934
- DOI: 10.1002/ijc.33540
Identifying key factors for the effectiveness of pancreatic cancer screening: A model-based analysis
Abstract
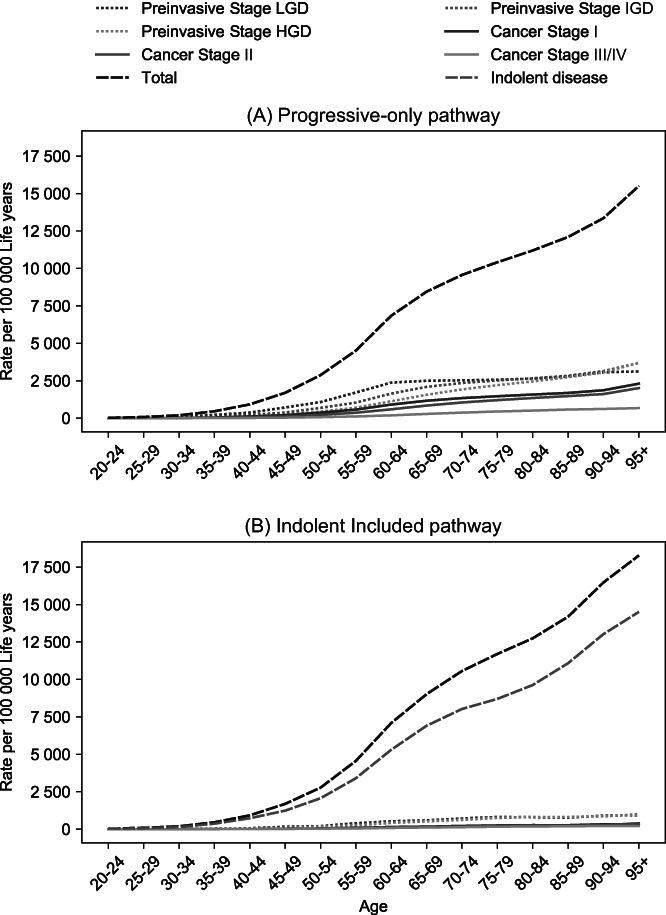
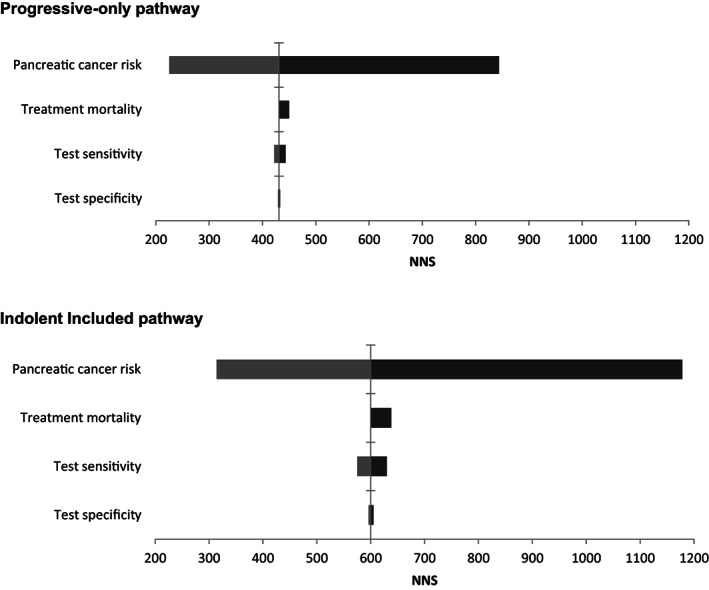
Pancreatic cancer (PC) survival is poor, as detection usually occurs late, when treatment options are limited. Screening of high-risk individuals may enable early detection and a more favorable prognosis. Knowledge gaps prohibit establishing the effectiveness of screening. We developed a Microsimulation Screening Analysis model to analyze the impact of relevant uncertainties on the effect of PC screening in high-risk individuals. The model simulates two base cases: one in which lesions always progress to PC and one in which indolent and faster progressive lesions coexist. For each base case, the effect of annual and 5-yearly screening with endoscopic ultrasonography/magnetic resonance imaging was evaluated. The impact of variance in PC risk, screening test characteristics and surgery-related mortality was evaluated using sensitivity analyses. Screening resulted in a reduction of PC mortality by at least 16% in all simulated scenarios. This reduction depended strongly on the natural disease course (annual screening: -57% for "Progressive-only" vs -41% for "Indolent Included"). The number of screen and surveillance tests needed to prevent one cancer death was impacted most by PC risk. A 10% increase in test sensitivity reduced mortality by 1.9% at most. Test specificity is important for the number of surveillance tests. In conclusion, screening reduces PC mortality in all modeled scenarios. The natural disease course and PC risk strongly determines the effectiveness of screening. Test sensitivity seems of lesser influence than specificity. Future research should gain more insight in PC pathobiology to establish the true value of PC screening in high-risk individuals.
Keywords: microsimulation model; pancreatic cancer; screening.
© 2021 The Authors. International Journal of Cancer published by John Wiley & Sons Ltd on behalf of Union for International Cancer Control.
Conflict of interest statement
The authors disclosed no potential conflicts of interest.
Figures

References
-
- Habbema JDF, Van Oortmarssen GJ, Lubbe JTN, Van der Maas PJ. The miscan simulation program for the evaluation of screening for disease. Comput Meth Prog Bio. 1985;20(1):79‐93. - PubMed
-
- Loeve F, Boer R, Zauber AG, et al. National polyp study data: evidence for regression of adenomas. Int J Cancer. 2004;111(4):633‐639. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
