

Transfer boarding delays care more in low-volume rural emergency departments: A cohort study
- PMID: 33644911
- PMCID: PMC8715860
- DOI: 10.1111/jrh.12559
Transfer boarding delays care more in low-volume rural emergency departments: A cohort study
Abstract
Purpose: Emergency department (ED) crowding is increasing and is associated with adverse patient outcomes. The objective of this study was to measure the relative impact of ED boarding on timeliness of early ED care for new patient arrivals, with a focus on the differential impact in low-volume rural hospitals.
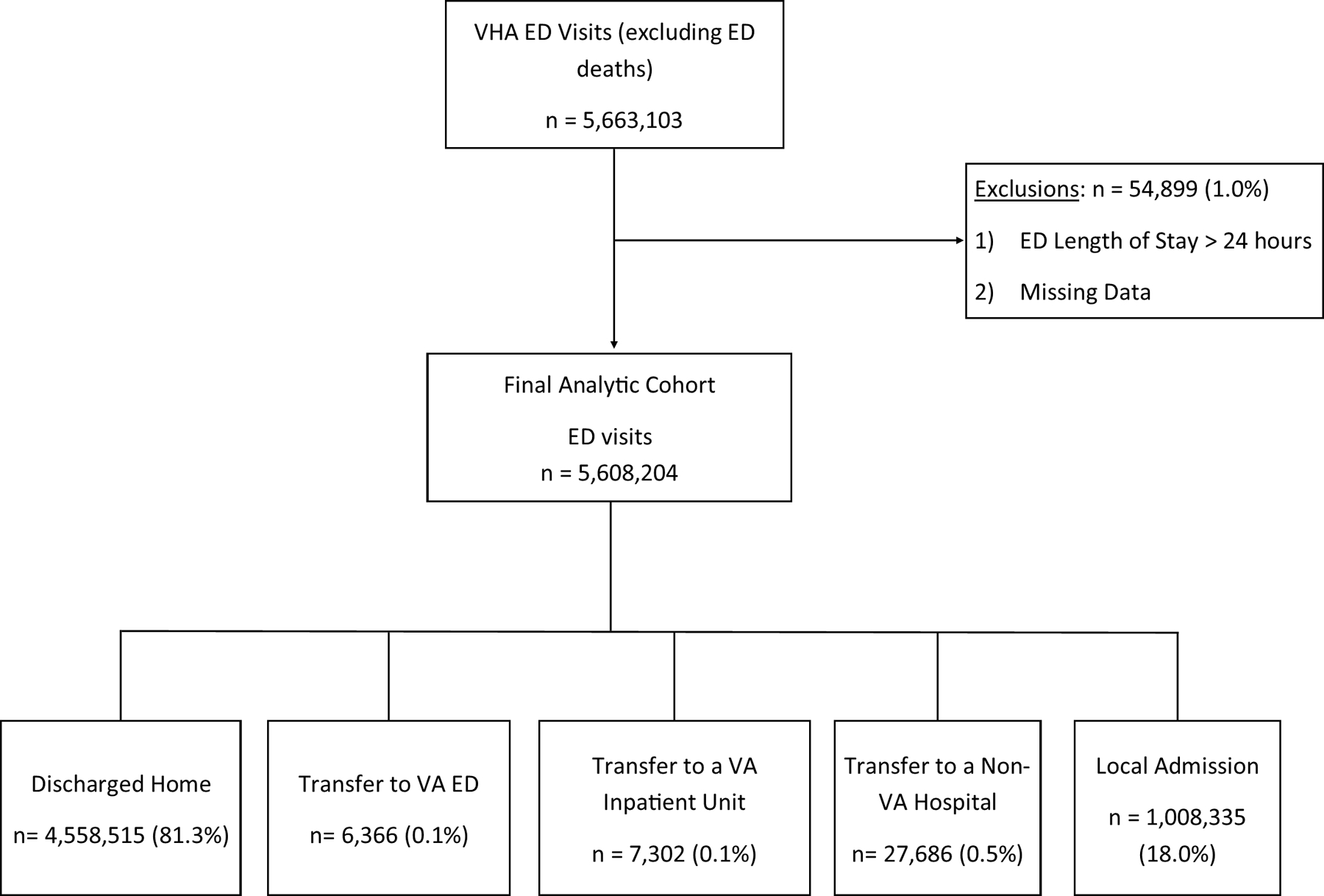
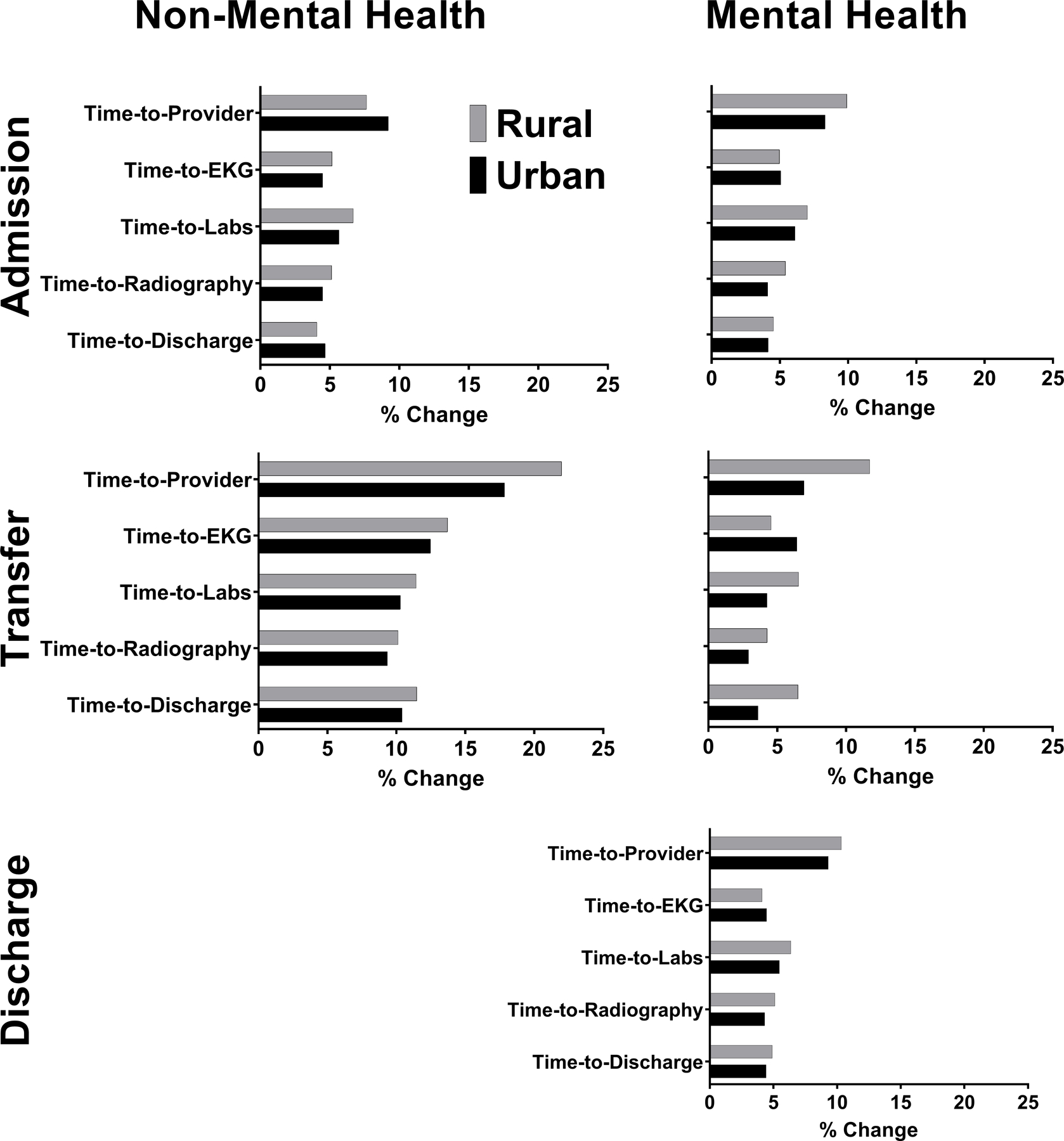
Methods: A retrospective cohort of all patients presenting to a Veterans Health Administration (VHA) ED between 2011 and 2014. The primary exposure was the number of patients in the ED at the time of ED registration, stratified by disposition (admit, discharge, or transfer) and mental health diagnosis. The primary outcome was time-to-provider evaluation, and secondary outcomes included time-to-EKG, time-to-laboratory testing, time-to-radiography, and total ED length-of-stay. Rurality was measured using the Rural-Urban Commuting Areas.
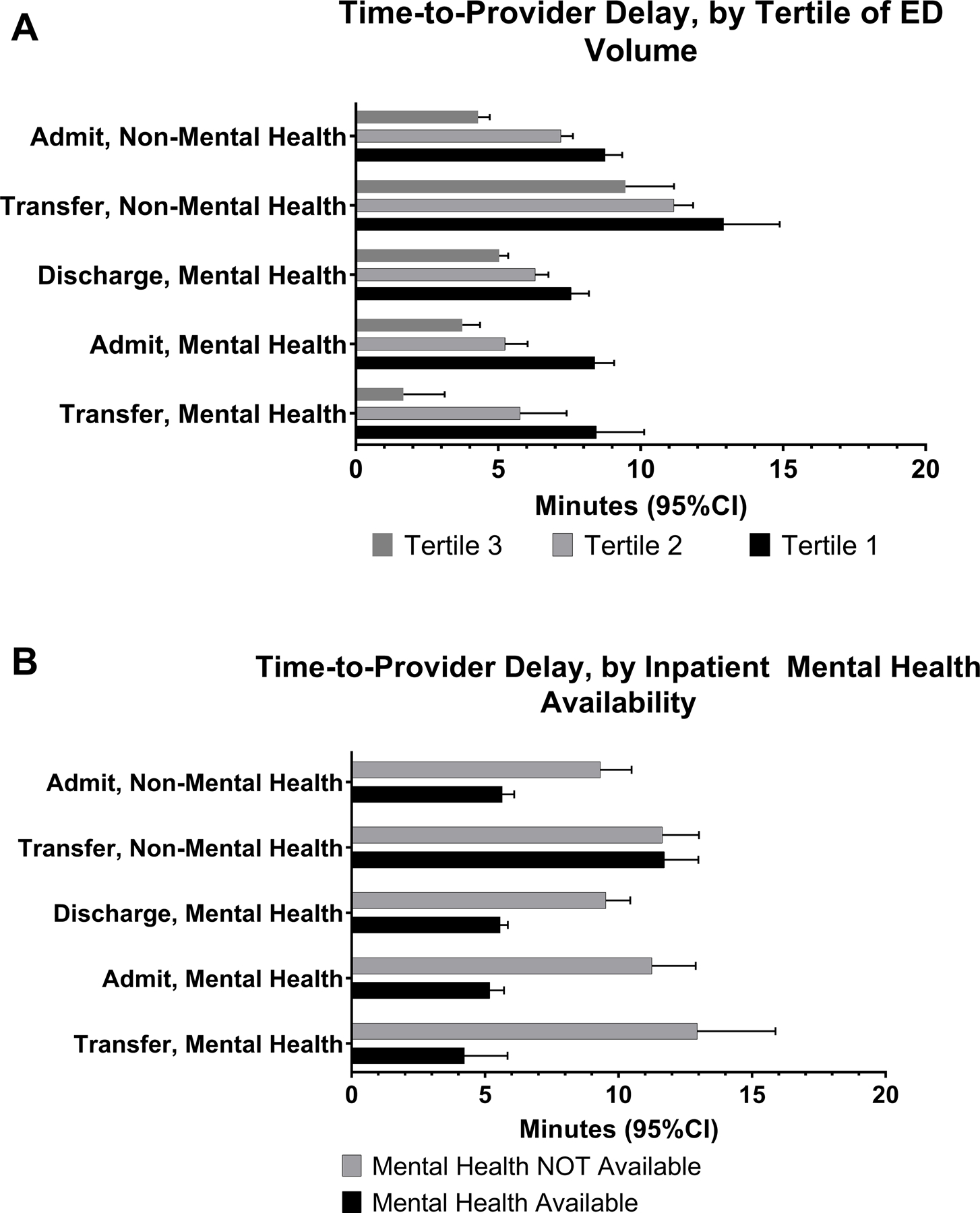
Findings: A total of 5,912,368 patients were included from all 123 VHA EDs. Adjusting for acuity, new patients had longer time-to-provider when more patients were in the ED, and patients awaiting transfer for nonmental health conditions impacted time-to-provider for new patients (16.6 min delays, 95% CI: 12.3-20.7 min) more than other patient types. Rural patients saw a greater impact of crowding on care timeliness than nonrural patients (additional 5.3 min in time-to-provider per additional patient in ED, 95% CI: 4.3-6.4), and the impact of additional patients in all categories was most pronounced in the lowest-volume EDs.
Conclusions: Patients seen in EDs with more crowding have small, but additive, delays in early elements of ED care, and transferring patients with nonmental health diagnoses from rural facilities were associated with the greatest impact.
Keywords: crowding; emergency service; hospitals; patient transfer; rural.
© 2021 National Rural Health Association.
Conflict of interest statement
Figures
Similar articles
-
Association of Emergency Department Length of Stay and Crowding for Patients with ST-Elevation Myocardial Infarction.West J Emerg Med. 2015 Dec;16(7):1067-72. doi: 10.5811/westjem.2015.8.27908. Epub 2015 Dec 16. West J Emerg Med. 2015. PMID: 26759656 Free PMC article.
-
Emergency Department Boarding, Inpatient Census, and Interhospital Transfer Acceptances.JAMA Netw Open. 2025 May 1;8(5):e2512299. doi: 10.1001/jamanetworkopen.2025.12299. JAMA Netw Open. 2025. PMID: 40434774 Free PMC article.
-
Telehealth Decreases Rural Emergency Department Wait Times for Behavioral Health Patients in a Group of Critical Access Hospitals.Telemed J E Health. 2019 Dec;25(12):1154-1164. doi: 10.1089/tmj.2018.0227. Epub 2019 Feb 8. Telemed J E Health. 2019. PMID: 30735100
-
Comparison of methods for measuring crowding and its effects on length of stay in the emergency department.Acad Emerg Med. 2011 Dec;18(12):1269-77. doi: 10.1111/j.1553-2712.2011.01232.x. Acad Emerg Med. 2011. PMID: 22168190 Review.
-
International perspectives on emergency department crowding.Acad Emerg Med. 2011 Dec;18(12):1358-70. doi: 10.1111/j.1553-2712.2011.01235.x. Acad Emerg Med. 2011. PMID: 22168200 Review.
References
-
- Rui PKK, Ashman JJ. . National Hospital Ambulatory Medical Care Survey: 2016 emergency department summary tables. 2016; https://www.cdc.gov/nchs/data/nhamcs/web_tables/2016_ed_web_tables.pdf.
-
- Thomas S, Pink G, Reiter K. Characteristics of Communites Served by Rural Hospitals Predicted to be at High Risk of Financial Distress in 2019 North Carolina Rural Health Research Program Findings Brief 2019.
-
- Rabin E, Kocher K, McClelland M, et al. Solutions To Emergency Department ‘Boarding’ And Crowding Are Underused And May Need To Be Legislated. Health Aff (Millwood) 2012;31(8):1757–1766. - PubMed
-
- Schneider SM, Gallery ME, Schafermeyer R, Zwemer FL. Emergency department crowding: A point in time. Annals of Emergency Medicine 2003;42(2):167–172. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
