

In Vivo Printing of Nanoenabled Scaffolds for the Treatment of Skeletal Muscle Injuries
- PMID: 33644996
- PMCID: PMC8137605
- DOI: 10.1002/adhm.202002152
In Vivo Printing of Nanoenabled Scaffolds for the Treatment of Skeletal Muscle Injuries
Abstract
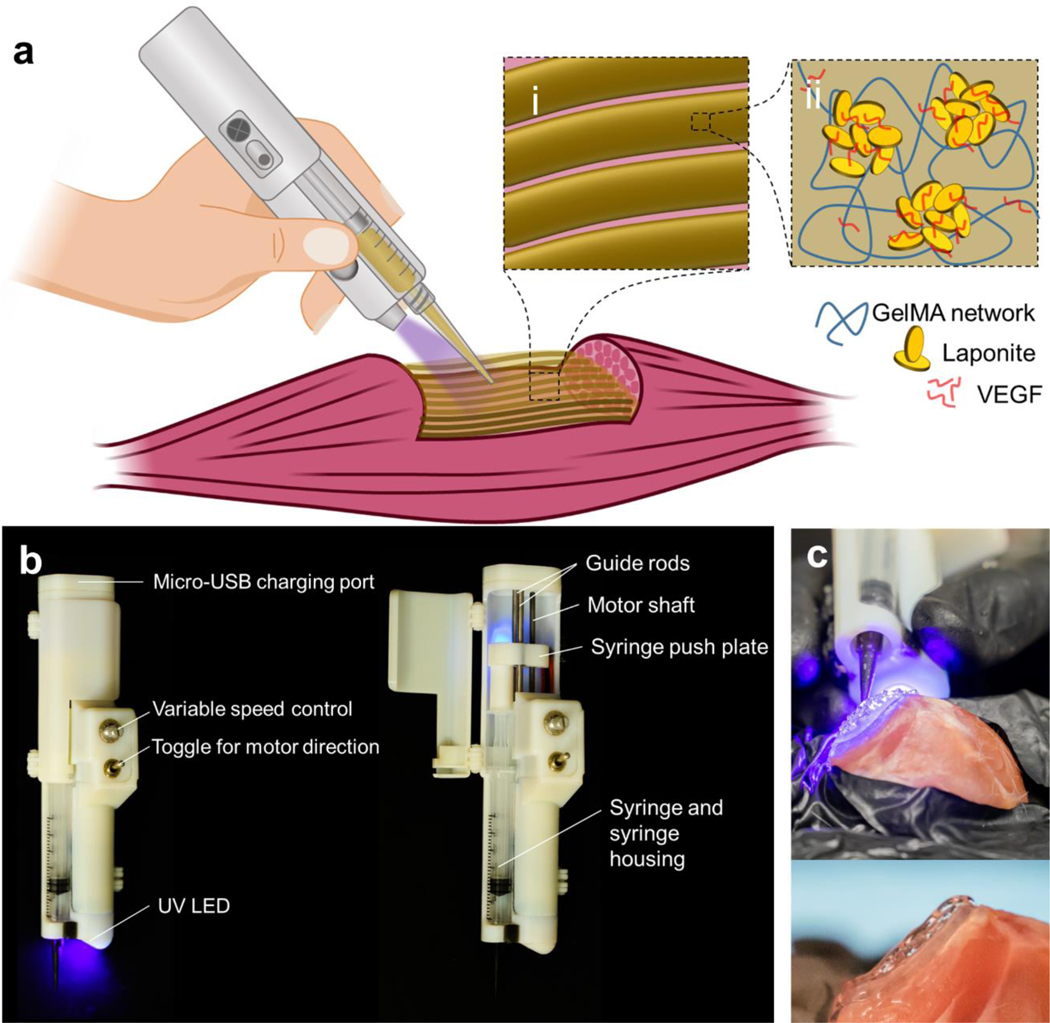
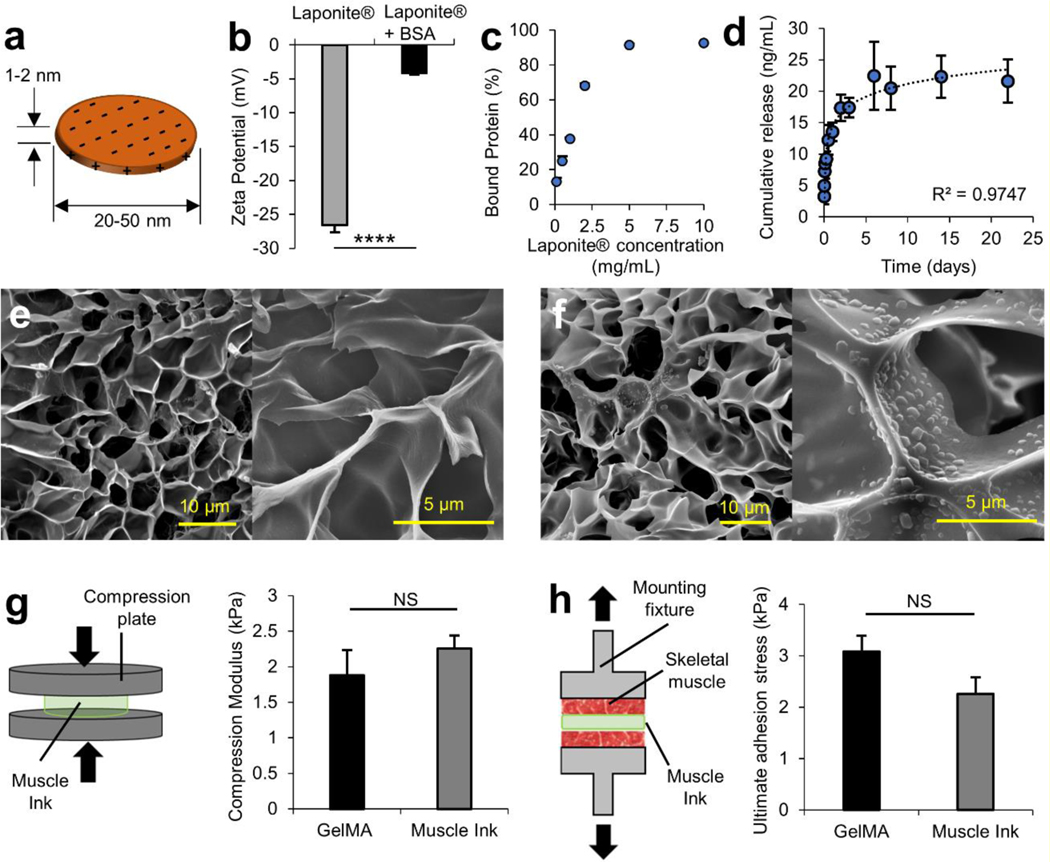
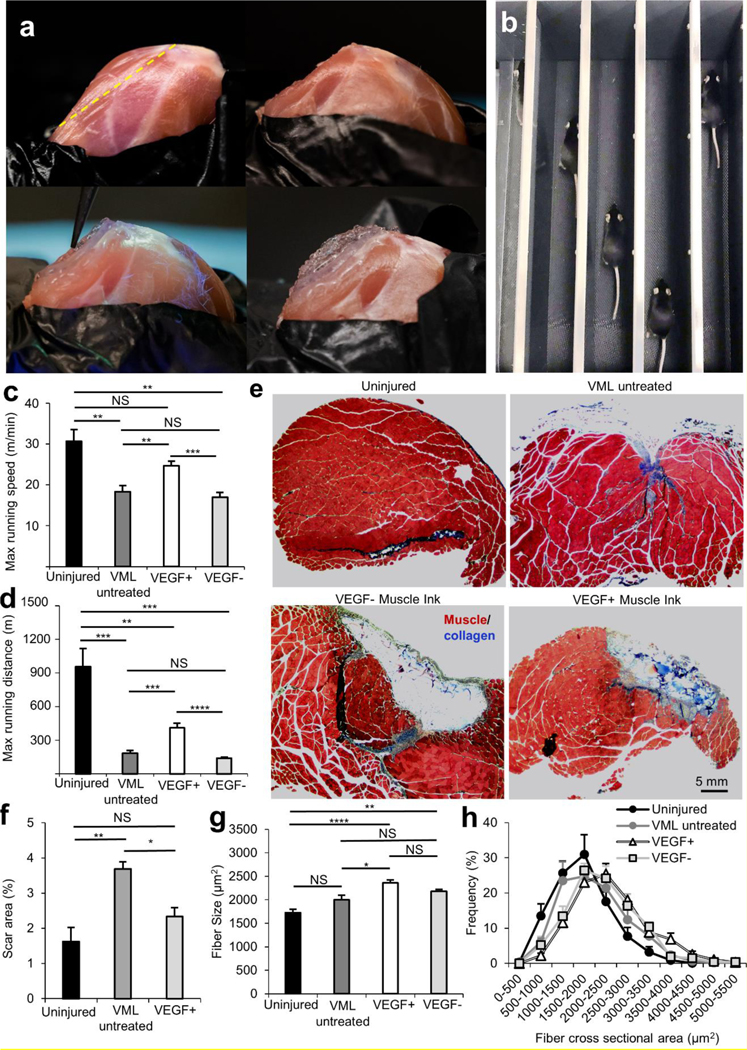
Extremity skeletal muscle injuries result in substantial disability. Current treatments fail to recoup muscle function, but properly designed and implemented tissue engineering and regenerative medicine techniques can overcome this challenge. In this study, a nanoengineered, growth factor-eluting bioink that utilizes Laponite nanoclay for the controlled release of vascular endothelial growth factor (VEGF) and a GelMA hydrogel for a supportive and adhesive scaffold that can be crosslinked in vivo is presented. The bioink is delivered with a partially automated handheld printer for the in vivo formation of an adhesive and 3D scaffold. The effect of the controlled delivery of VEGF alone or paired with adhesive, supportive, and fibrilar architecture has not been studied in volumetric muscle loss (VML) injuries. Upon direct in vivo printing, the constructs are adherent to skeletal muscle and sustained release of VEGF. The in vivo printing of muscle ink in a murine model of VML injury promotes functional muscle recovery, reduced fibrosis, and increased anabolic response compared to untreated mice. The in vivo construction of a therapeutic-eluting 3D scaffold paves the way for the immediate treatment of a variety of soft tissue traumas.
Keywords: functional recovery; handheld printers; hydrogel scaffolds; in vivo printing; soft tissue injuries; volumetric muscle loss.
© 2021 Wiley-VCH GmbH.
Figures

References
-
- Nuutila K, Sakthivel D, Kruse C, Tran P, Giatsidis G, Sinha I, Wound repair and regeneration : official publication of the Wound Healing Society [and] the European Tissue Repair Society 2017, 25, 408. - PubMed
-
- Grogan BF, Hsu JR, The Journal of the American Academy of Orthopaedic Surgeons 2011, 19 Suppl 1, S35. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
