

The burden of non-communicable diseases and mortality in people living with HIV (PLHIV) in the pre-, early- and late-HAART era
- PMID: 33645000
- PMCID: PMC8247855
- DOI: 10.1111/hiv.13077
The burden of non-communicable diseases and mortality in people living with HIV (PLHIV) in the pre-, early- and late-HAART era
Abstract
Objectives: To estimate the burden of non-communicable diseases (NCDs) and mortality among PLHIV in the pre-, early- and late-HAART (highly active antiretroviral therapy) era.
Methods: We conducted a cohort study using population-based Danish medical registries including all adult HIV-infected residents of the Central Denmark Region during 1985-2017. For each HIV patient, we selected 10 comparisons from the background population matched by age, sex and municipality of residence. Based on hospital-related diagnoses we estimated the prevalence and incidence of specific NCD at diagnosis and at 5 and 10 years.
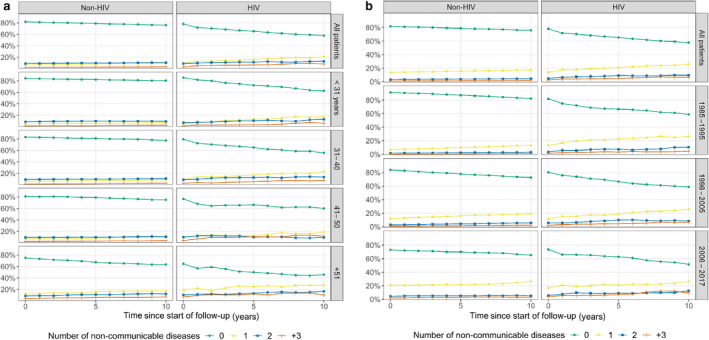
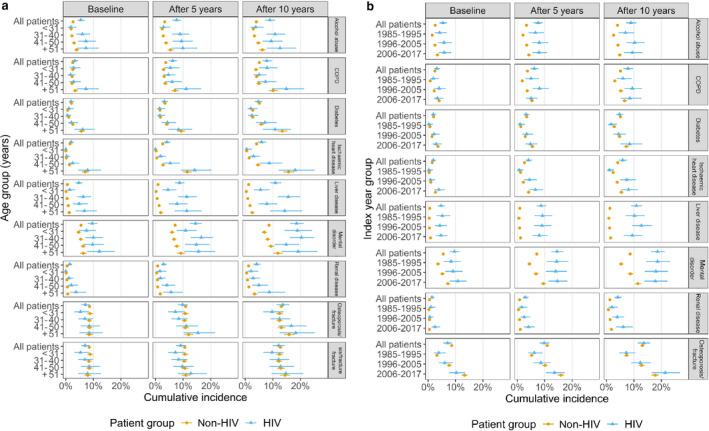
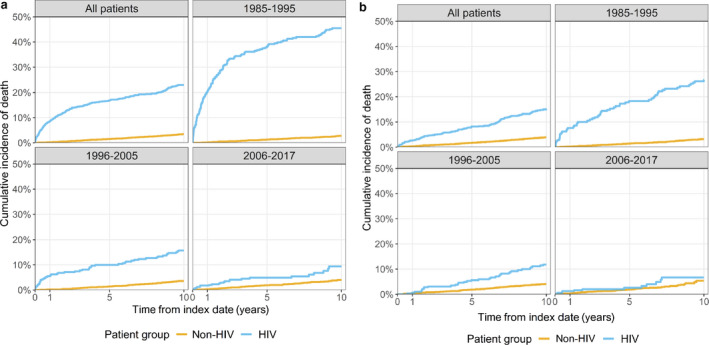
Results: We identified 1043 PLHIV and 10 430 matched comparisons. PLHIV had lower socioeconomic status and more were born outside western Europe. At HIV diagnosis, 21.9% of PHLIV vs. 18.2% of non-HIV individuals had at least one NCD, increasing to 42.2% vs. 25.9% after 10 years. PLHIV had higher prevalence and cumulative incidence of alcohol abuse, chronic obstructive pulmonary disease (COPD), ischaemic heart disease, mental disorders, renal and liver disease, but no increased risk of diabetes mellitus. Only PLHIV in the age groups 41-50 and > 51 years had an increased incidence of osteoporosis. From the pre- to the late-HAART era, 10-year mortality among PLHIV decreased from 45.5% to 9.4% but continued at more than twice that of uninfected comparisons. However, in the late-HAART era, the mortality of PLHIV who were alive 2 years after HIV diagnosis was approaching that of comparisons.
Conclusions: Even in the late-HAART era, PLHIV have an excess mortality, which may be attributable to several NCDs being more prevalent among PLHIV. The prevalence rates of ischaemic heart disease, diabetes, osteoporosis and renal disease tend to increase over calendar time. Therefore, improvement of survival and quality of life of PLHIV neets strategies to reduce the risk of developing NCDs, including avoiding toxic antiretroviral therapy and lifestyle changes.
Keywords: HIV; chronic obstructive pulmonary disease; diabetes mellitus; ischaemic heart disease; liver disease; mental disorders; mortality; non-communicable diseases; osteoporosis; renal disease.
© 2021 The Authors. HIV Medicine published by John Wiley & Sons Ltd on behalf of British HIV Association.
Figures
References
-
- Lohse N, Obel N. Update of survival for persons with HIV infection in Denmark. Ann Intern Med 2016; 165: 749–750. - PubMed
-
- Legarth RA, Ahlstrom MG, Kronborg G et al. Long‐term mortality in HIV‐infected individuals 50 years or older: a nationwide, population‐based cohort study. J Acquir Immune Defic Syndr 2016; 71: 213–218. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
