

Theatre ventilation
- PMID: 33645287
- PMCID: PMC9157996
- DOI: 10.1308/rcsann.2020.7146
Theatre ventilation
Abstract
Introduction: Owing to the COVID-19 pandemic, there has been significant disruption to all surgical specialties. In the UK, units have cancelled elective surgery and a decrease in aerosol generating procedures (AGPs) was favoured. Centres around the world advocate the use of negative pressure environments for AGPs in reducing the spread of infectious airborne particles. We present an overview of operating theatre ventilation systems and the respective evidence with relation to surgical site infection (SSI) and airborne pathogen transmission in light of COVID-19.
Methods: A literature search was conducted using the PubMed, Cochrane Library and MEDLINE databases. Search terms included "COVID-19", "theatre ventilation", "laminar", "turbulent" and "negative pressure".
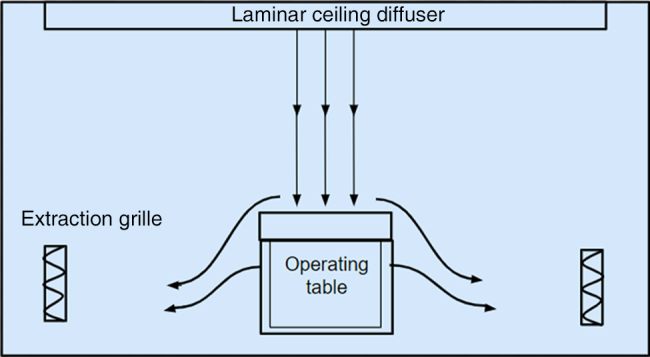
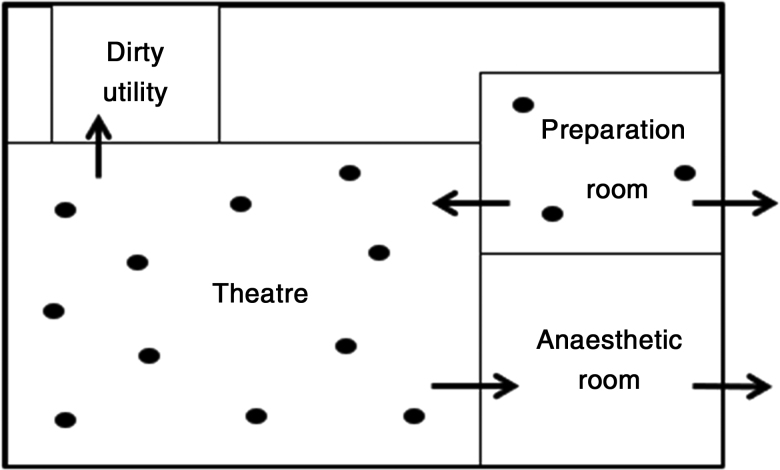
Findings: Evidence for laminar flow ventilation in reducing the rate of SSI in orthopaedic surgery is widely documented. There is little evidence to support its use in general surgery. Following previous viral outbreaks, some centres have introduced negative pressure ventilation in an attempt to decrease exposure of airborne pathogens to staff and surrounding areas. This has again been suggested during the COVID-19 pandemic. A limited number of studies show some positive results for the use of negative pressure ventilation systems and reduction in spread of pathogens; however, cost, accessibility and duration of conversion remain an unexplored issue. Overall, there is insufficient evidence to advocate large scale conversion at this time. Nevertheless, it may be useful for each centre to have its own negative pressure room available for AGPs and high risk patients.
Keywords: COVID-19; Coronavirus; General surgery; Laminar flow; Operating room; SARS.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous