

Effect of a Multifaceted Clinical Pharmacist Intervention on Medication Safety After Hospitalization in Persons Prescribed High-risk Medications: A Randomized Clinical Trial
- PMID: 33646267
- PMCID: PMC7922235
- DOI: 10.1001/jamainternmed.2020.9285
Effect of a Multifaceted Clinical Pharmacist Intervention on Medication Safety After Hospitalization in Persons Prescribed High-risk Medications: A Randomized Clinical Trial
Erratum in
-
Error in Figure Value.JAMA Intern Med. 2021 May 1;181(5):727. doi: 10.1001/jamainternmed.2021.2050. JAMA Intern Med. 2021. PMID: 33938926 Free PMC article. No abstract available.
Abstract
Importance: The National Action Plan for Adverse Drug Event (ADE) Prevention identified 3 high-priority, high-risk drug classes as targets for reducing the risk of drug-related injuries: anticoagulants, diabetes agents, and opioids.
Objective: To determine whether a multifaceted clinical pharmacist intervention improves medication safety for patients who are discharged from the hospital and prescribed medications within 1 or more of these high-risk drug classes.
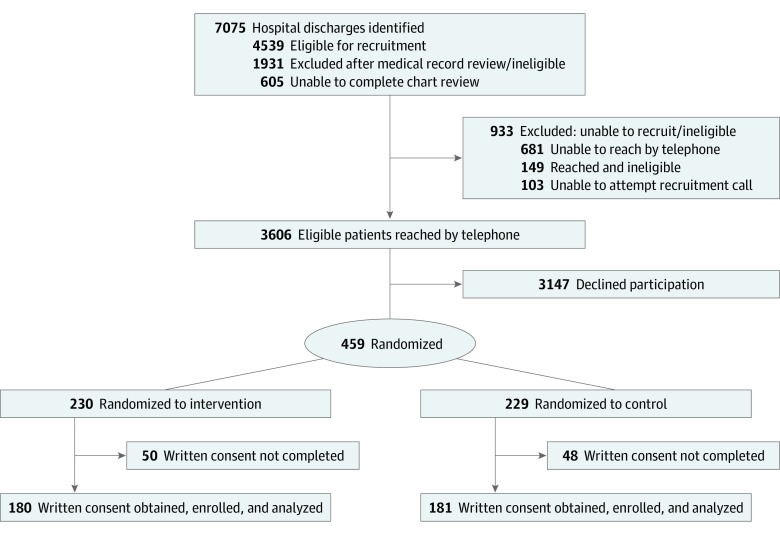
Design, setting, and participants: This randomized clinical trial was conducted at a large multidisciplinary group practice in Massachusetts and included patients 50 years or older who were discharged from the hospital and prescribed at least 1 high-risk medication. Participants were enrolled into the trial from June 2016 through September 2018.
Interventions: The pharmacist-directed intervention included an in-home assessment by a clinical pharmacist, evidence-based educational resources, communication with the primary care team, and telephone follow-up. Participants in the control group were provided educational materials via mail.
Main outcomes and measures: The study assessed 2 outcomes over a 45-day posthospital discharge period: (1) adverse drug-related incidents and (2) a subset defined as clinically important medication errors, which included preventable or ameliorable ADEs and potential ADEs (ie, medication-related errors that may not yet have caused injury to a patient, but have the potential to cause future harm if not addressed). Clinically important medication errors were the primary study outcome.
Results: There were 361 participants (mean [SD] age, 68.7 [9.3] years; 177 women [49.0%]; 319 White [88.4%] and 8 Black individuals [2.2%]). Of these, 180 (49.9%) were randomly assigned to the intervention group and 181 (50.1%) to the control group. Among all participants, 100 (27.7%) experienced 1 or more adverse drug-related incidents, and 65 (18%) experienced 1 or more clinically important medication errors. There were 81 adverse drug-related incidents identified in the intervention group and 72 in the control group. There were 44 clinically important medication errors in the intervention group and 45 in the control group. The intervention did not significantly alter the per-patient rate of adverse drug-related incidents (unadjusted incidence rate ratio, 1.13; 95% CI, 0.83-1.56) or clinically important medication errors (unadjusted incidence rate ratio, 0.99; 95% CI, 0.65-1.49).
Conclusions and relevance: In this randomized clinical trial, there was not an observed lower rate of adverse drug-related incidents or clinically important medication errors during the posthospitalization period that was associated with a clinical pharmacist intervention. However, there were study recruitment challenges and lower than expected numbers of events among the study population.
Trial registration: ClinicalTrials.gov Identifier: NCT02781662.
Conflict of interest statement
Figures
Comment in
-
Adverse Drug Events After Hospitalization-Are We Missing the Mark?JAMA Intern Med. 2021 May 1;181(5):618-619. doi: 10.1001/jamainternmed.2020.9282. JAMA Intern Med. 2021. PMID: 33646266 Free PMC article. No abstract available.
References
-
- US Department of Health and Human Services Office of Disease Prevention and Health Promotion . National action plan for adverse drug event prevention. Accessed January 12, 2015. http://www.health.gov/hai/pdfs/ADE-Action-Plan-508c.pdf
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
