

[Overtreatment in intensive care medicine-recognition, designation, and avoidance : Position paper of the Ethics Section of the DIVI and the Ethics section of the DGIIN]
- PMID: 33646332
- PMCID: PMC7919250
- DOI: 10.1007/s00063-021-00794-4
[Overtreatment in intensive care medicine-recognition, designation, and avoidance : Position paper of the Ethics Section of the DIVI and the Ethics section of the DGIIN]
Abstract
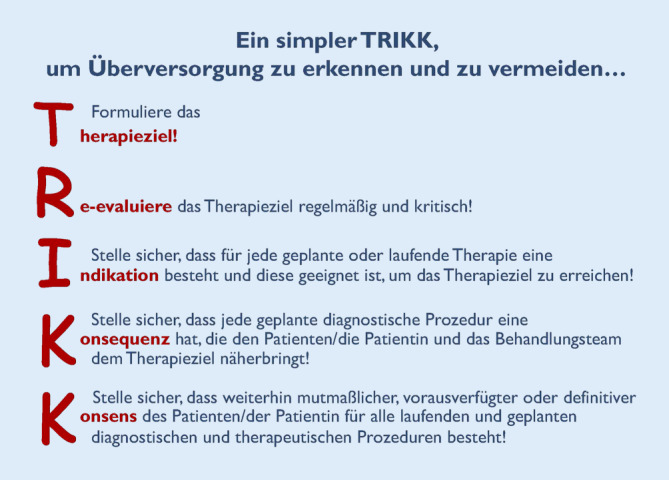
Despite social laws, overtreatment, undertreatment, and incorrect treatment are all present in the German health care system. Overtreatment denotes diagnostic and therapeutic measures that are not appropriate because they do not improve the patients' length or quality of life, cause more harm than benefit, and/or are not consented to by the patient. Overtreatment can result in considerable burden for patients, their families, the treating teams, and society. This position paper describes causes of overtreatment in intensive care medicine and makes specific recommendations to identify and prevent it. Recognition and avoidance of overtreatment in intensive care medicine requires measures on the micro-, meso- and macrolevels, especially the following: (1) frequent (re-)evaluation of the therapeutic goal within the treating team while taking the patient's will into consideration, while simultaneously attending to the patients and their families; (2) fostering a patient-centered corporate culture in the hospital, giving priority to high-quality patient care; (3) minimizing improper incentives in health care financing, supported by reform of the reimbursement system that is still based on diagnose-related groups; (4) strengthening of interprofessional co-operation via education and training; and (5) initiating and advancing a societal discourse on overtreatment.
Ungeachtet der sozialgesetzlichen Vorgaben existieren im deutschen Gesundheitssystem in der Patientenversorgung nebeneinander Unter‑, Fehl- und Überversorgung. Überversorgung bezeichnet diagnostische und therapeutische Maßnahmen, die nicht angemessen sind, da sie die Lebensdauer oder Lebensqualität der Patienten nicht verbessern, mehr Schaden als Nutzen verursachen und/oder von den Patienten nicht gewollt werden. Daraus können hohe Belastungen für die Patienten, deren Familien, die Behandlungsteams und die Gesellschaft resultieren. Dieses Positionspapier erläutert Ursachen von Überversorgung in der Intensivmedizin und gibt differenzierte Empfehlungen zu ihrer Erkennung und Vermeidung. Zur Erkennung und Vermeidung von Überversorgung in der Intensivmedizin erfordert es Maßnahmen auf der Mikro‑, Meso- und Makroebene, insbesondere die folgenden: 1) regelmäßige Evaluierung des Therapieziels im Behandlungsteam unter Berücksichtigung des Patientenwillens und unter Begleitung von Patienten und Angehörigen; 2) Förderung einer patientenzentrierten Unternehmenskultur im Krankenhaus mit Vorrang einer qualitativ hochwertigen Patientenversorgung; 3) Minimierung von Fehlanreizen im Krankenhausfinanzierungssystem gestützt auf die notwendige Reformierung des fallpauschalbasierten Vergütungssystems; 4) Stärkung der interdisziplinären/interprofessionellen Zusammenarbeit in Aus‑, Fort- und Weiterbildung; 5) Initiierung und Begleitung eines gesellschaftlichen Diskurses zur Überversorgung.
Keywords: End of life care; Extent of treatment; Patient care; Patient preference; Therapeutic goal.

References
-
- Adler K, Schlieper D, Kindgen-Milles D, et al. Integration der Palliativmedizin in die Intensivmedizin : Systematische Ubersichtsarbeit. Anaesthesist. 2017;66:660–666. - PubMed
-
- Au SS, Couillard P, Roze des Ordons A, et al. Outcomes of ethics consultations in adult ICus: a systematic review and meta-analysis. Crit Care Med. 2018;46:799–808. - PubMed
-
- Beinersdorf A. Der Informationsverlust bei der Patientenverlegung. intensiv. 2007;15:268–273.
-
- Bion J, Antonelli M, Blanch L, et al. White paper: statement on conflicts of interest. Intensive Care Med. 2018;44:1657–1668. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
