

Major bleeding complications in critically ill patients with COVID-19 pneumonia
- PMID: 33646501
- PMCID: PMC7919235
- DOI: 10.1007/s11239-021-02403-9
Major bleeding complications in critically ill patients with COVID-19 pneumonia
Abstract
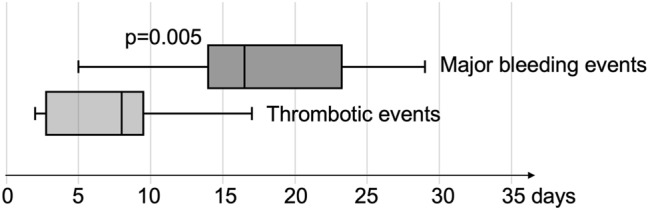
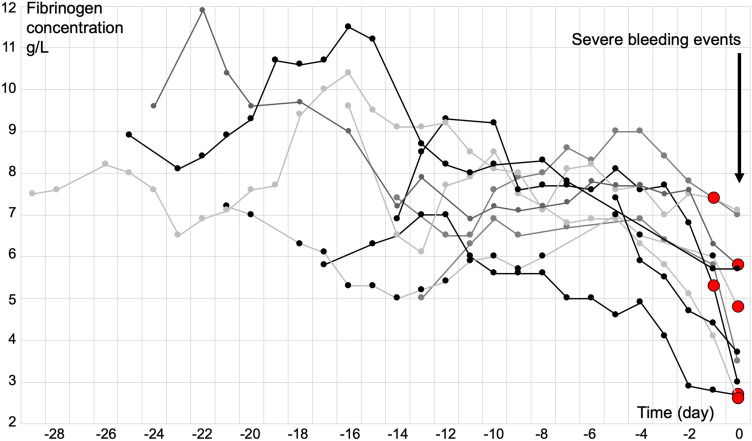
As patients with COVID-19 pneumonia admitted to intensive care unit (ICU) have high rates of thrombosis, high doses of thromboprophylaxis have been proposed. The associated bleeding risk remains unknown. We investigated major bleeding complications in ICU COVID-19 patients and we examined their relationship with inflammation and thromboprophylaxis. Retrospective monocentric study of consecutive adult patients admitted in ICU for COVID-19 pneumonia requiring mechanical ventilation. Data collected included demographics, anticoagulation status, coagulation tests and outcomes including major bleeding and thrombotic events. Among 56 ICU COVID-19 patients, 10 (18%) patients had major bleeding and 16 (29%) thrombotic events. Major bleeding occurred later than thrombosis after ICU admission [17(14-23) days versus 9(3-11) days respectively (p = 0.005)]. Fibrinogen concentration always decreased several days [4(3-5) days] before bleeding; D-dimers followed the same trend. All bleeding patients were treated with anticoagulants and anticoagulation was overdosed for 6 (60%) patients on the day of bleeding or the day before. In the whole cohort, overdose was measured in 22 and 78% of patients receiving therapeutic anticoagulation during fibrinogen increase and decrease respectively (p < 0.05). Coagulation disorders had biphasic evolution during COVID-19: first thrombotic events during initial hyperinflammation, then bleeding events once inflammation reduced, as confirmed by fibrinogen and D-dimers decrease. Most bleeding events complicated heparin overdose, promoted by inflammation decrease, suggesting to carefully monitor heparin during COVID-19. Thromboprophylaxis may be adapted to this biphasic evolution, with initial high doses reduced to standard doses once the high thrombotic risk period ends and fibrinogen decreases, to prevent bleeding events.
Keywords: Anticoagulant; Bleeding; COVID-19; Fibrinogen; Inflammation; Thrombosis.
© 2021. The Author(s), under exclusive licence to Springer Science+Business Media, LLC part of Springer Nature.
Conflict of interest statement
AGo: honoraria and travel fees from Bayer-Healthcare, Boehringer-Ingelheim, Bristol-Myers-Squibb/Pfizer and Sanofi. Other authors declares that they have no conflict of interest.
Figures
References
-
- Poissy J, Goutay J, Caplan M, Parmentier E, Duburcq T, Lassalle F, Jeanpierre E, Rauch A, Labreuche J, Susen S, Lille ICU Haemostasis COVID-19 Group Pulmonary embolism in patients with COVID-19: awareness of an increased prevalence. Circulation. 2020;142:184–186. doi: 10.1161/CIRCULATIONAHA.120.047430. - DOI - PubMed
-
- Ackermann M, Verleden SE, Kuehnel M, Haverich A, Welte T, Laenger F, Vanstapel A, Werlein C, Stark H, Tzankov A, Li WW, Li VW, Mentzer SJ, Jonigk D. Pulmonary vascular endothelialitis, thrombosis, and angiogenesis in COVID-19. N Engl J Med. 2020;383:120–128. doi: 10.1056/NEJMoa2015432. - DOI - PMC - PubMed
-
- Rauch A, Labreuche J, Lassalle F, Goutay J, Caplan M, Charbonnier L, Rohn A, Jeanpierre E, Dupont A, Duhamel A, Faure K, Lambert M, Kipnis E, Garrigue D, Lenting PJ, Poissy J, Susen S. Coagulation biomarkers are independent predictors of increased oxygen requirements in COVID-19. J Thromb Haemost. 2020;18(11):2942–2953. doi: 10.1111/jth.15067. - DOI - PMC - PubMed
-
- Rosovsky RP, Sanfilippo KM, Wang TF, Rajan SK, Shah S, Martin KA, Ní Áinle F, Huisman M, Hunt BJ, Kahn SR, Kevane B, Lee AY, McLintock C, Baumann KL. Anticoagulation practice patterns in COVID-19: a global survey. Res Pract Thromb Haemost. 2020;4:969–983. doi: 10.1002/rth2.12414. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
