

Lung ultrasound presentation of COVID-19 patients: phenotypes and correlations
- PMID: 33646508
- PMCID: PMC7917171
- DOI: 10.1007/s11739-020-02620-9
Lung ultrasound presentation of COVID-19 patients: phenotypes and correlations
Abstract
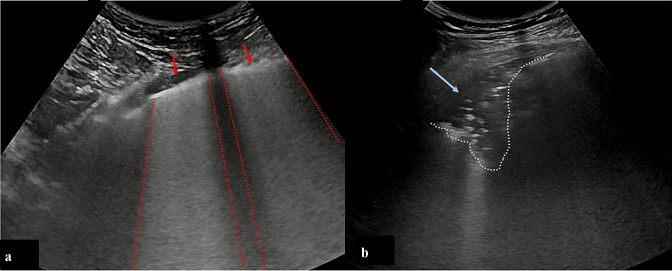
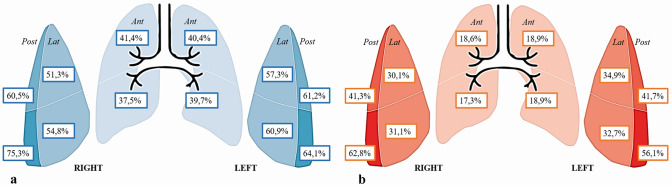
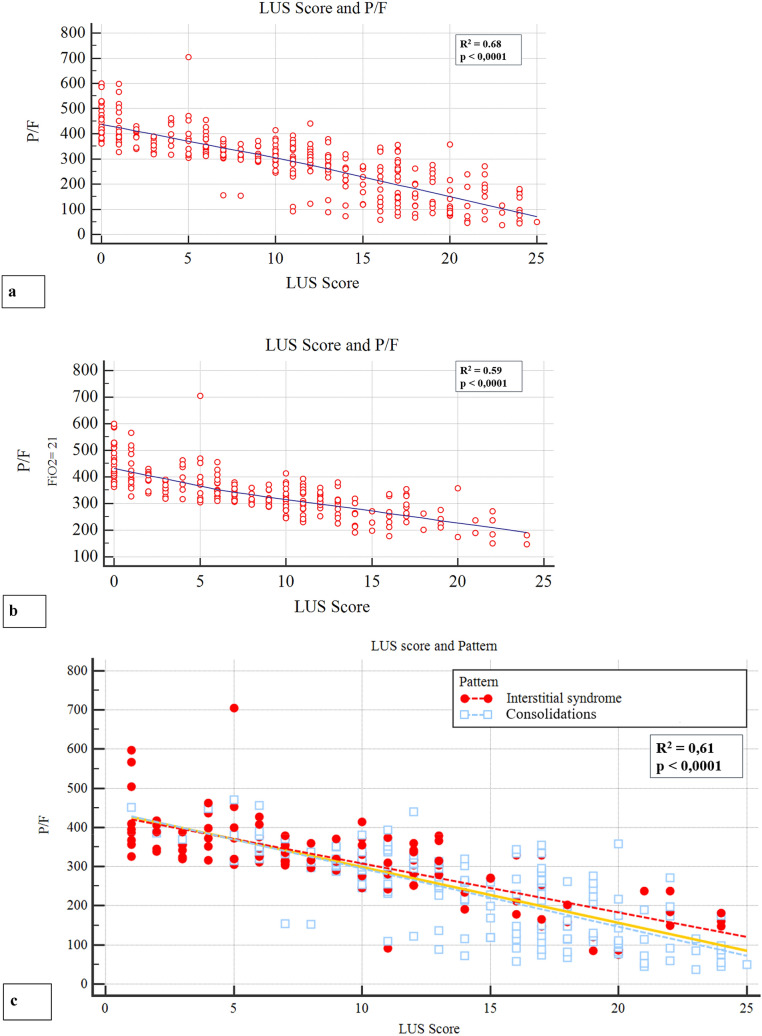
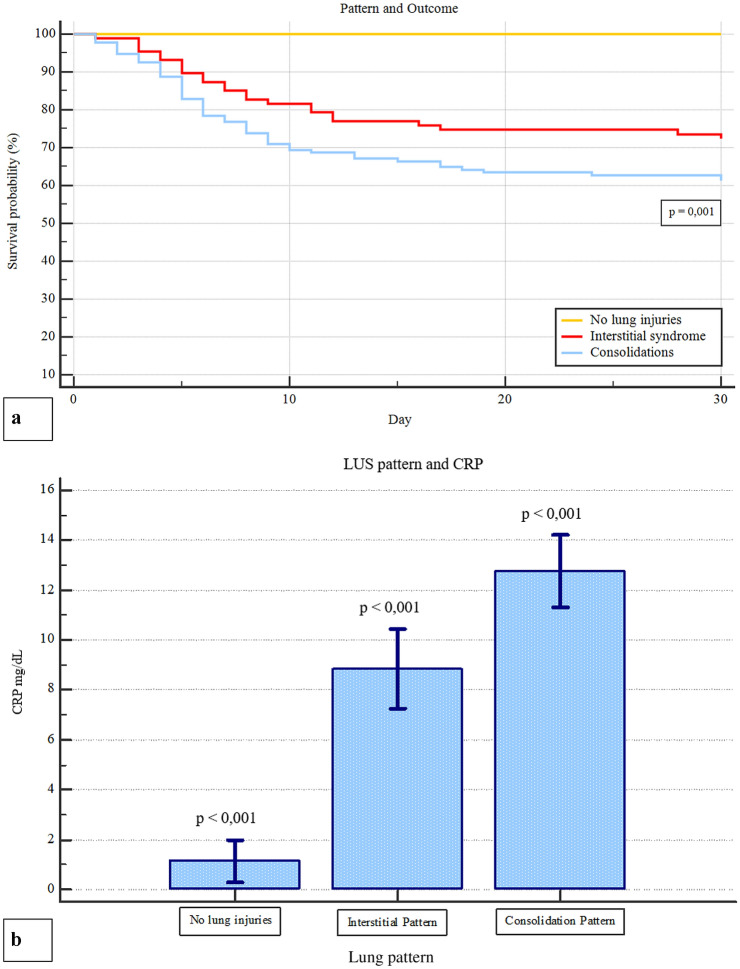
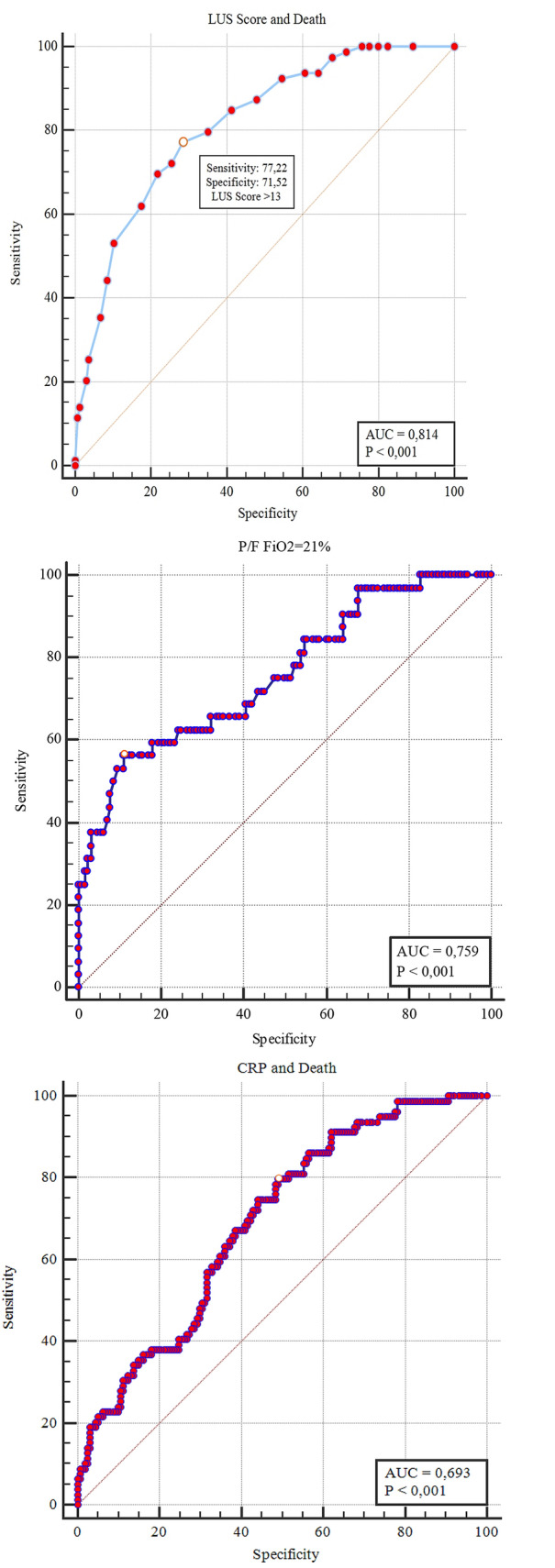
Bedside lung ultrasound (LUS) can play a role in the setting of the SarsCoV2 pneumonia pandemic. To evaluate the clinical and LUS features of COVID-19 in the ED and their potential prognostic role, a cohort of laboratory-confirmed COVID-19 patients underwent LUS upon admission in the ED. LUS score was derived from 12 fields. A prevalent LUS pattern was assigned depending on the presence of interstitial syndrome only (Interstitial Pattern), or evidence of subpleural consolidations in at least two fields (Consolidation Pattern). The endpoint was 30-day mortality. The relationship between hemogasanalysis parameters and LUS score was also evaluated. Out of 312 patients, only 36 (11.5%) did not present lung involvment, as defined by LUS score < 1. The majority of patients were admitted either in a general ward (53.8%) or in intensive care unit (9.6%), whereas 106 patients (33.9%) were discharged from the ED. In-hospital mortality was 25.3%, and 30-day survival was 67.6%. A LUS score > 13 had a 77.2% sensitivity and a 71.5% specificity (AUC 0.814; p < 0.001) in predicting mortality. LUS alterations were more frequent (64%) in the posterior lower fields. LUS score was related with P/F (R2 0.68; p < 0.0001) and P/F at FiO2 = 21% (R2 0.59; p < 0.0001). The correlation between LUS score and P/F was not influenced by the prevalent ultrasound pattern. LUS represents an effective tool in both defining diagnosis and stratifying prognosis of COVID-19 pneumonia. The correlation between LUS and hemogasanalysis parameters underscores its role in evaluating lung structure and function.
Keywords: COVID-19; Echographic phenotypes; Interstitial pneumonia; LUS score; Lung ultrasound.
© 2021. The Author(s).
Conflict of interest statement
FM received fees for lectures from GE Healthcare, Hamilton Medical, SEDA SpA. A research agreement is active between University of Pavia and Hamilton Medical.
Figures
Comment in
-
Lung ultrasound presentation of covid-19 patients: phenotypes and correlations-comment.Intern Emerg Med. 2021 Aug;16(5):1417-1418. doi: 10.1007/s11739-021-02777-x. Epub 2021 May 31. Intern Emerg Med. 2021. PMID: 34056696 Free PMC article. No abstract available.
Comment on
-
COVID-19 pneumonia: different respiratory treatments for different phenotypes?Intensive Care Med. 2020 Jun;46(6):1099-1102. doi: 10.1007/s00134-020-06033-2. Epub 2020 Apr 14. Intensive Care Med. 2020. PMID: 32291463 Free PMC article. No abstract available.
-
COVID-19 pneumonia: ARDS or not?Crit Care. 2020 Apr 16;24(1):154. doi: 10.1186/s13054-020-02880-z. Crit Care. 2020. PMID: 32299472 Free PMC article. No abstract available.
References
-
- Center JHCR coronavirus.jhu.edu/map.html
-
- Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He JX, Liu L, Shan H, Lei CL, Hui DSC, Du B, Li LJ, Zeng G, Yuen KY, Chen RC, Tang CL, Wang T, Chen PY, Xiang J, Li SY, Wang JL, Liang ZJ, Peng YX, Wei L, Liu Y, Hu YH, Peng P, Wang JM, Liu JY, Chen Z, Li G, Zheng ZJ, Qiu SQ, Luo J, Ye CJ, Zhu SY, Zhong NS; China Medical Treatment Expert Group for C (2020) Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
