

Effect of empagliflozin on ectopic fat stores and myocardial energetics in type 2 diabetes: the EMPACEF study
- PMID: 33648515
- PMCID: PMC7919089
- DOI: 10.1186/s12933-021-01237-2
Effect of empagliflozin on ectopic fat stores and myocardial energetics in type 2 diabetes: the EMPACEF study
Abstract
Background: Empagliflozin is a sodium-glucose cotransporter 2 (SGLT2) inhibitor that has demonstrated cardiovascular and renal protection in patients with type 2 diabetes (T2D). We hypothesized that empaglifozin (EMPA) could modulate ectopic fat stores and myocardial energetics in high-fat-high-sucrose (HFHS) diet mice and in type 2 diabetics (T2D).
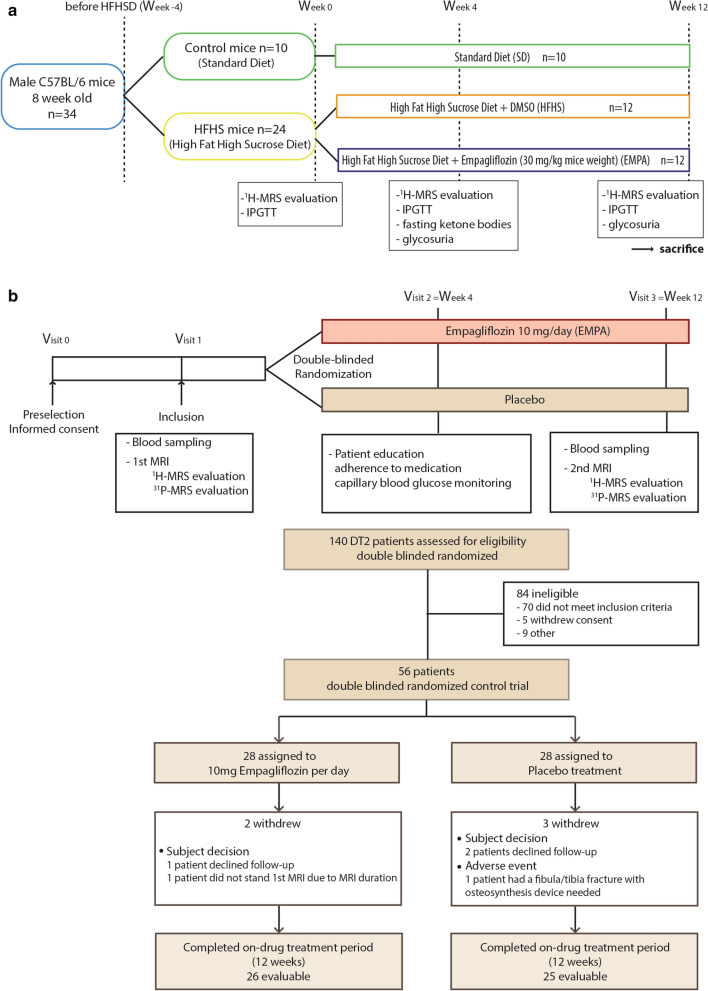
Methods: C57BL/6 HFHS mice (n = 24) and T2D subjects (n = 56) were randomly assigned to 12 weeks of treatment with EMPA (30 mg/kg in mice, 10 mg/day in humans) or with placebo. A 4.7 T or 3 T MRI with 1H-MRS evaluation-myocardial fat (primary endpoint) and liver fat content (LFC)-were performed at baseline and at 12 weeks. In humans, standard cardiac MRI was coupled with myocardial energetics (PCr/ATP) measured with 31P-MRS. Subcutaneous (SAT) abdominal, visceral (VAT), epicardial and pancreatic fat were also evaluated. The primary efficacy endpoint was the change in epicardial fat volume between EMPA and placebo from baseline to 12 weeks. Secondary endpoints were the differences in PCr/ATP ratio, myocardial, liver and pancreatic fat content, SAT and VAT between groups at 12 weeks.
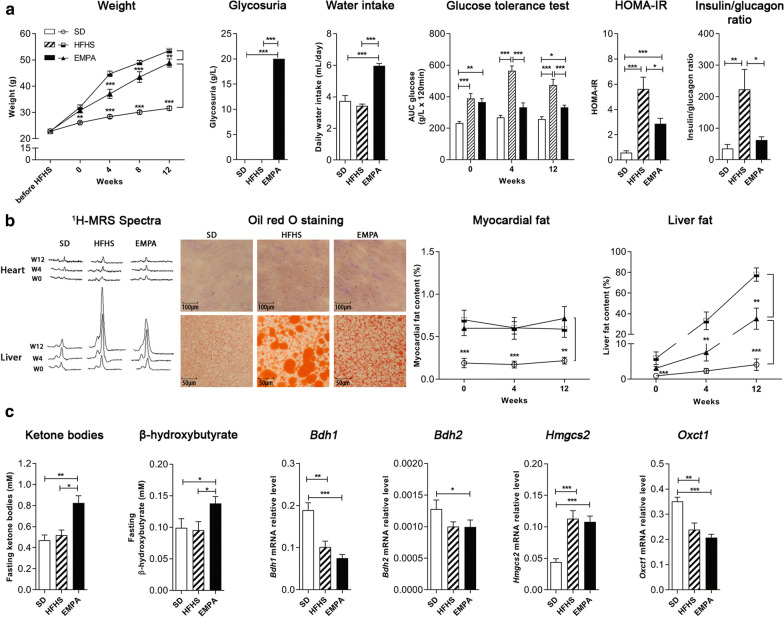
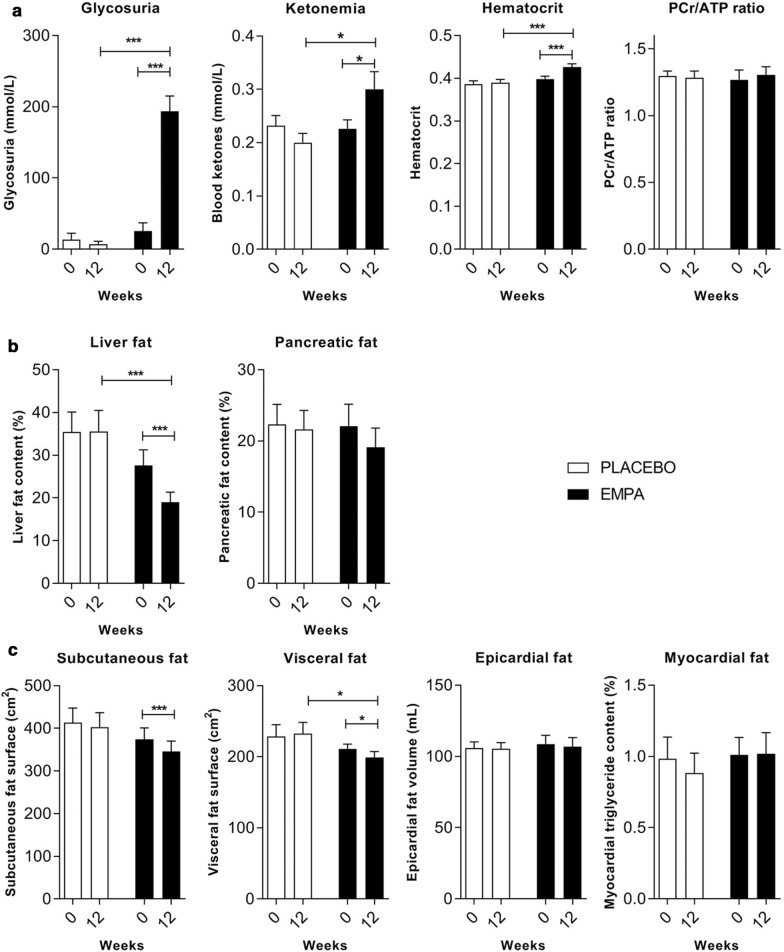
Results: In mice fed HFHS, EMPA significantly improved glucose tolerance and increased blood ketone bodies (KB) and β-hydroxybutyrate levels (p < 0.05) compared to placebo. Mice fed HFHS had increased myocardial and liver fat content compared to standard diet mice. EMPA significantly attenuated liver fat content by 55%, (p < 0.001) but had no effect on myocardial fat. In the human study, all the 56 patients had normal LV function with mean LVEF = 63.4 ± 7.9%. Compared to placebo, T2D patients treated with EMPA significantly lost weight (- 2.6 kg [- 1.2; - 3.7]) and improved their HbA1c by 0.88 ± 0.74%. Hematocrit and EPO levels were significantly increased in the EMPA group compared to placebo (p < 0.0001, p = 0.041). EMPA significantly increased glycosuria and plasma KB levels compared to placebo (p < 0.0001, p = 0.012, respectively), and significantly reduced liver fat content (- 27 ± 23 vs. - 2 ± 24%, p = 0.0005) and visceral fat (- 7.8% [- 15.3; - 5.6] vs. - 0.1% [- 1.1;6.5], p = 0.043), but had no effect on myocardial or epicardial fat. At 12 weeks, no significant change was observed in the myocardial PCr/ATP (p = 0.57 between groups).
Conclusions: EMPA effectively reduced liver fat in mice and humans without changing epicardial, myocardial fat or myocardial energetics, rebutting the thrifty substrate hypothesis for cardiovascular protection of SGLT2 inhibitors. Trial registration NCT, NCT03118336. Registered 18 April 2017, https://clinicaltrials.gov/ct2/show/NCT03118336.
Keywords: 31P-MRS; Ectopic fat; Epicardial adipose tissue; MRI; Myocardial energetics; Pcr/atp; SGLT2 inhibitors.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Lee H-C, Shiou Y-L, Jhuo S-J, Chang C-Y, Liu P-L, Jhuang W-J, et al. The sodium-glucose co-transporter 2 inhibitor empagliflozin attenuates cardiac fibrosis and improves ventricular hemodynamics in hypertensive heart failure rats. Cardiovasc Diabetol. 2019;18:45. doi: 10.1186/s12933-019-0849-6. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
