

Imaging modalities in pregnant cancer patients
- PMID: 33649009
- PMCID: PMC7925814
- DOI: 10.1136/ijgc-2020-001779
Imaging modalities in pregnant cancer patients
Abstract
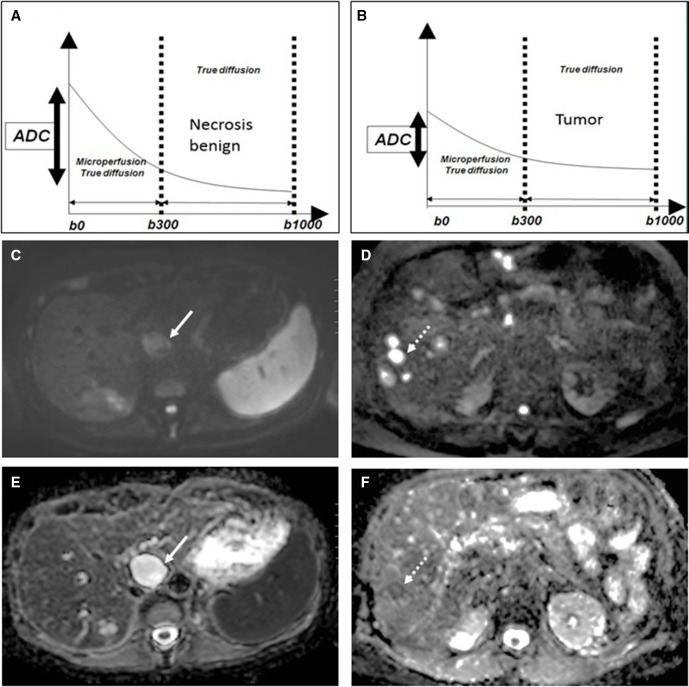
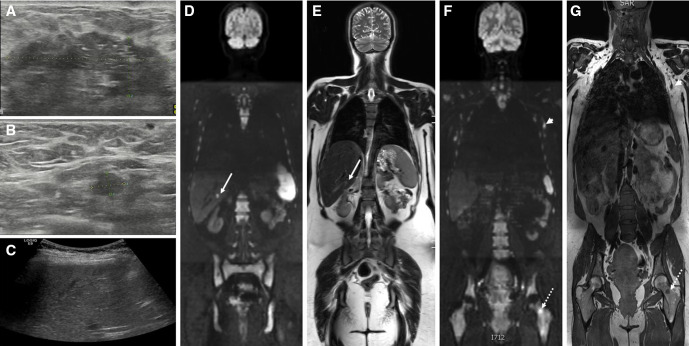
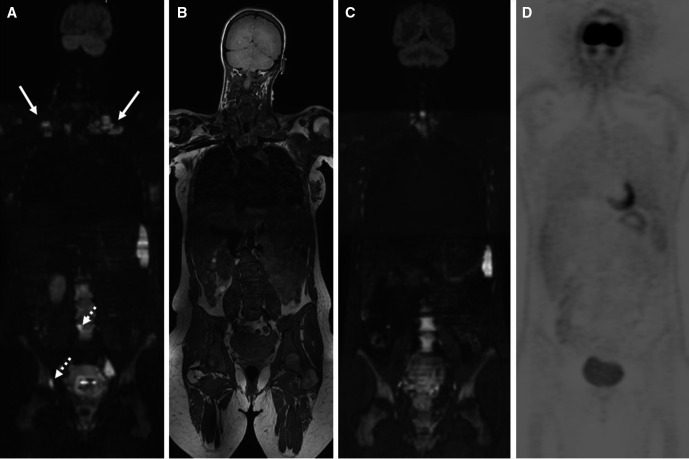
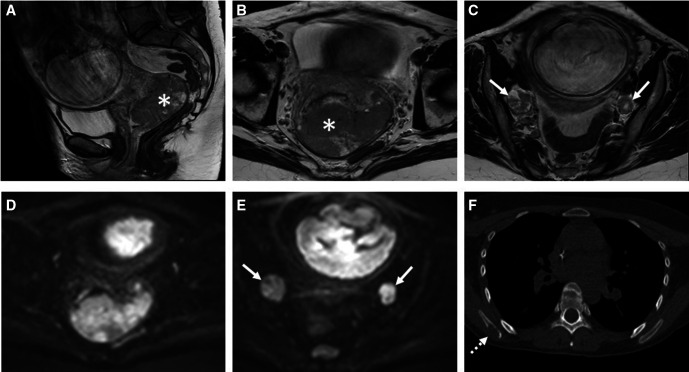
Cancer during pregnancy is increasingly diagnosed due to the trend of delaying pregnancy to a later age and probably also because of increased use of non-invasive prenatal testing for fetal aneuploidy screening with incidental finding of maternal cancer. Pregnant women pose higher challenges in imaging, diagnosis, and staging of cancer. Physiological tissue changes related to pregnancy makes image interpretation more difficult. Moreover, uncertainty about the safety of imaging modalities, fear of (unnecessary) fetal radiation, and lack of standardized imaging protocols may result in underutilization of the necessary imaging tests resulting in suboptimal staging. Due to the absence of radiation exposure, ultrasound and MRI are obvious first-line imaging modalities for detailed locoregional disease assessment. MRI has the added advantage of a more reproducible comprehensive organ or body region assessment, the ability of distant staging through whole-body evaluation, and the combination of anatomical and functional information by diffusion-weighted imaging which obviates the need for a gadolinium-based contrast-agent. Imaging modalities with inherent radiation exposure such as CT and nuclear imaging should only be performed when the maternal benefit outweighs fetal risk. The cumulative radiation exposure should not exceed the fetal radiation threshold of 100 mGy. Imaging should only be performed when necessary for diagnosis and likely to guide or change management. Radiologists play an important role in the multidisciplinary team in order to select the most optimal imaging strategies that balance maternal benefit with fetal risk and that are most likely to guide treatment decisions. Our aim is to provide an overview of possibilities and concerns in current clinical applications and developments in the imaging of patients with cancer during pregnancy.
Keywords: interventional; neoplasm metastasis; neoplasms; radiology.
© IGCS and ESGO 2021. Re-use permitted under CC BY-NC. No commercial re-use. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Difficulties with diagnosis of malignancies in pregnancy.Best Pract Res Clin Obstet Gynaecol. 2016 May;33:19-32. doi: 10.1016/j.bpobgyn.2015.10.005. Epub 2015 Oct 19. Best Pract Res Clin Obstet Gynaecol. 2016. PMID: 26586541 Review.
-
Fetal Radiation Dose from 18F-FDG in Pregnant Patients Imaged with PET, PET/CT, and PET/MR.J Nucl Med. 2015 Aug;56(8):1218-22. doi: 10.2967/jnumed.115.157032. Epub 2015 Jun 18. J Nucl Med. 2015. PMID: 26089550
-
Prenatal screening for fetal aneuploidy in singleton pregnancies.J Obstet Gynaecol Can. 2011 Jul;33(7):736-750. doi: 10.1016/S1701-2163(16)34961-1. J Obstet Gynaecol Can. 2011. PMID: 21749752
-
Imaging modalities and optimized imaging protocols in pregnant patients with cancer.Abdom Radiol (NY). 2023 May;48(5):1579-1589. doi: 10.1007/s00261-023-03798-0. Epub 2023 Jan 23. Abdom Radiol (NY). 2023. PMID: 36688976 Review.
-
Ionising radiation-free whole-body MRI versus (18)F-fluorodeoxyglucose PET/CT scans for children and young adults with cancer: a prospective, non-randomised, single-centre study.Lancet Oncol. 2014 Mar;15(3):275-85. doi: 10.1016/S1470-2045(14)70021-X. Epub 2014 Feb 19. Lancet Oncol. 2014. PMID: 24559803
Cited by
-
Cancer in pregnancy: overview and epidemiology.Abdom Radiol (NY). 2023 May;48(5):1559-1563. doi: 10.1007/s00261-022-03633-y. Epub 2022 Aug 12. Abdom Radiol (NY). 2023. PMID: 35960309 Review.
-
Cancer and Pregnancy: A Comprehensive Review.Cancers (Basel). 2021 Jun 18;13(12):3048. doi: 10.3390/cancers13123048. Cancers (Basel). 2021. PMID: 34207252 Free PMC article. Review.
-
Cervical cancer in the pregnant population.Abdom Radiol (NY). 2023 May;48(5):1679-1693. doi: 10.1007/s00261-023-03836-x. Epub 2023 Apr 18. Abdom Radiol (NY). 2023. PMID: 37071123 Review.
-
Cancer and Pregnancy in the Post-Roe v. Wade Era: A Comprehensive Review.Curr Oncol. 2023 Oct 25;30(11):9448-9457. doi: 10.3390/curroncol30110684. Curr Oncol. 2023. PMID: 37999104 Free PMC article. Review.
-
Pregnant patient with Xp11.2/transcription factor E3 translocation renal cell carcinoma: a case report and literature review.Front Oncol. 2024 Jun 26;14:1388880. doi: 10.3389/fonc.2024.1388880. eCollection 2024. Front Oncol. 2024. PMID: 38988705 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
