

Obstructive spirometry pattern and the risk of chronic kidney disease: analysis from the community-based prospective Ansan-Ansung cohort in Korea
- PMID: 33649059
- PMCID: PMC8098974
- DOI: 10.1136/bmjopen-2020-043432
Obstructive spirometry pattern and the risk of chronic kidney disease: analysis from the community-based prospective Ansan-Ansung cohort in Korea
Abstract
Objective: There have been limited studies on the relationship between obstructive spirometry pattern and the development of chronic kidney disease (CKD). We investigated the association between obstructive spirometry pattern and incident CKD development in a large-scale prospective cohort study.
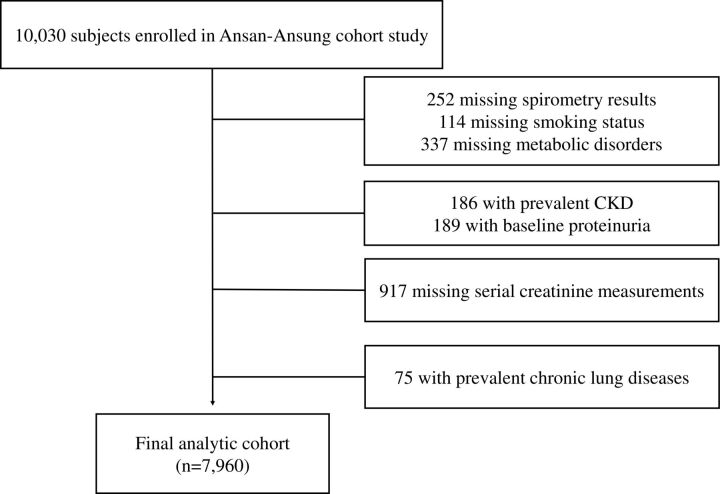
Methods: We reviewed the data of 7960 non-CKD adults aged 40-69 years who participated in the Ansung-Ansan cohort, a prospective community-based cohort study. Prebronchodilation results for the ratio of forced expiratory volume per 1 s (FEV1) to forced vital capacity (FVC) were used as the primary exposure. The primary outcome was incident CKD, defined as the first event of an estimated glomerular filtration rate <60 mL/min/1.73 m2. HRs and 95% CIs were calculated using multivariate Cox proportional hazard regression analysis.
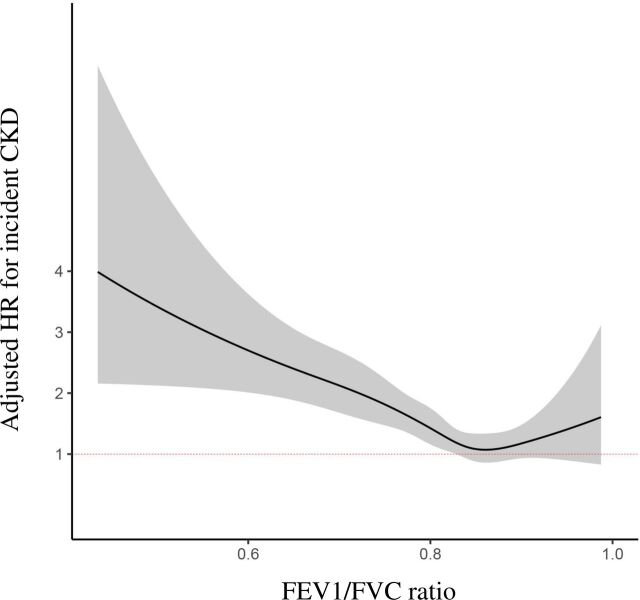
Results: Over a mean follow-up period of 11.7 years, incident CKD developed in 511 subjects (6.4%). An increase of 0.1 in FEV1/FVC was associated with a decreased risk of incident CKD (HR 0.76, 95% CI 0.68 to 0.84, p<0.001). Compared with the fourth quartile, the HR (95 % CI) of the first quartile of FEV1/FVC ratio was 1.81 (1.39 to 2.36, p<0.001). In the restricted cubic spline curve, the renal hazard associated with a decreased FEV1/FVC ratio was evident at FEV1/FVC values <0.80, showing a U-shaped relationship. In subgroup analysis, the renal hazard associated with a decreased FEV1/FVC ratio was particularly evident in people without metabolic syndrome (p for interaction=0.018).
Conclusion: Decreased FEV1/FVC ratio was independently associated with an increased risk of incident CKD development, particularly in people without metabolic syndrome. Future studies need to be conducted to confirm these results.
Keywords: chronic airways disease; chronic renal failure; respiratory physiology.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures


Similar articles
-
Association between measures of kidney function and preserved ratio impaired spirometry in diabetes: NHANES 2007-2012.BMJ Open. 2024 Nov 1;14(10):e075955. doi: 10.1136/bmjopen-2023-075955. BMJ Open. 2024. PMID: 39486815 Free PMC article.
-
Lung Function and Incident Kidney Disease: The Atherosclerosis Risk in Communities (ARIC) Study.Am J Kidney Dis. 2017 Nov;70(5):675-685. doi: 10.1053/j.ajkd.2017.05.021. Epub 2017 Jul 26. Am J Kidney Dis. 2017. PMID: 28754455 Free PMC article.
-
Relationship between airway obstruction and C-reactive protein levels in a community-based population of Korea.Int J Tuberc Lung Dis. 2019 Nov 1;23(11):1228-1234. doi: 10.5588/ijtld.18.0848. Int J Tuberc Lung Dis. 2019. PMID: 31718761
-
A Meta-analysis of Arsenic Exposure and Lung Function: Is There Evidence of Restrictive or Obstructive Lung Disease?Curr Environ Health Rep. 2018 Jun;5(2):244-254. doi: 10.1007/s40572-018-0192-1. Curr Environ Health Rep. 2018. PMID: 29637476 Free PMC article. Review.
-
[Progress in preserved ratio impaired spirometry].Zhonghua Jie He He Hu Xi Za Zhi. 2022 Oct 12;45(10):1046-1050. doi: 10.3760/cma.j.cn112147-20220518-00426. Zhonghua Jie He He Hu Xi Za Zhi. 2022. PMID: 36207961 Review. Chinese.
Cited by
-
Association between measures of kidney function and preserved ratio impaired spirometry in diabetes: NHANES 2007-2012.BMJ Open. 2024 Nov 1;14(10):e075955. doi: 10.1136/bmjopen-2023-075955. BMJ Open. 2024. PMID: 39486815 Free PMC article.
-
Lung Dysfunction and Chronic Kidney Disease: A Complex Network of Multiple Interactions.J Pers Med. 2023 Feb 3;13(2):286. doi: 10.3390/jpm13020286. J Pers Med. 2023. PMID: 36836520 Free PMC article. Review.
-
Strength, power and aerobic capacity of transgender athletes: a cross-sectional study.Br J Sports Med. 2024 May 28;58(11):586-597. doi: 10.1136/bjsports-2023-108029. Br J Sports Med. 2024. PMID: 38599680 Free PMC article.
-
Preserved ratio impaired spirometry, airflow obstruction, and their trajectories in relationship to chronic kidney disease: a prospective cohort study.Sci Rep. 2025 Jan 27;15(1):3439. doi: 10.1038/s41598-025-86952-6. Sci Rep. 2025. PMID: 39870785 Free PMC article.
References
-
- Barreiro TJ, Perillo I. An approach to interpreting spirometry. Am Fam Physician 2004;69:1107–14. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical