

Robotic transduodenal ampullectomy: Case report and review of the literature
- PMID: 33649269
- PMCID: PMC7952669
- DOI: 10.14701/ahbps.2021.25.1.150
Robotic transduodenal ampullectomy: Case report and review of the literature
Abstract
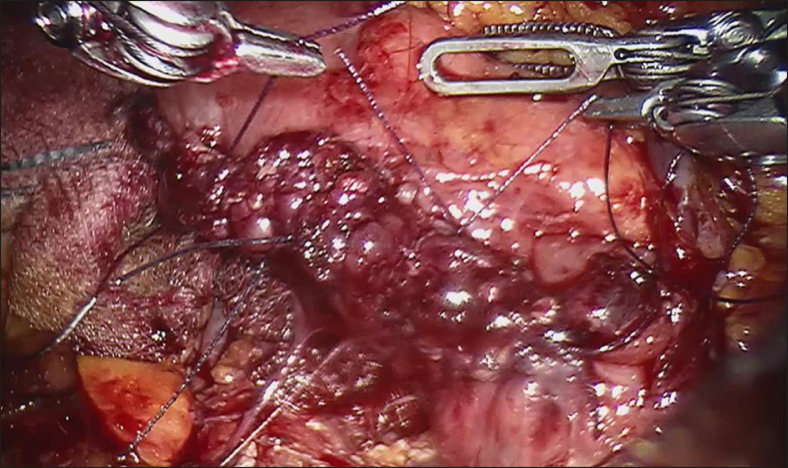
Ampullary neoplasms are relatively uncommon lesions with a risk of progression to malignancy. Depending on its nature, size and location, it may be best treated with endoscopic papillotomy, pancreaticoduodenectomy or transduodenal ampullectomy. Transduodenal ampullectomy offers a higher chance of complete resection compared to endoscopic papillotomy, and carries lower morbidity than a pancreaticoduodenectomy, making it the ideal choice for localised ampullary tumour not involving the ducts but not amenable to complete endoscopic resection. While traditionally performed via open surgery, it has been attempted via laparoscopic approach and more recently robotic approach. We present a case of a 63-year-old man who underwent a robotic transduodenal ampullectomy for ampullary adenoma with high grade dysplasia, and review the literature surrounding robotic transduodenal ampullectomy.
Keywords: Ampullary neoplasm; Minimally invasive surgery; Robotic surgery; Transduodenal ampullectomy.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures






References
-
- Halsted WS. Contributions to the surgery of the bile passages, especially of the common bile-duct. Boston Med Surg J. 1899;141:645–654. doi: 10.1056/NEJM189912281412601. - DOI
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources