

Very High Coronary Artery Calcium (≥1000) and Association With Cardiovascular Disease Events, Non-Cardiovascular Disease Outcomes, and Mortality: Results From MESA
- PMID: 33650435
- PMCID: PMC8058297
- DOI: 10.1161/CIRCULATIONAHA.120.050545
Very High Coronary Artery Calcium (≥1000) and Association With Cardiovascular Disease Events, Non-Cardiovascular Disease Outcomes, and Mortality: Results From MESA
Abstract
Background: There are limited data on the unique cardiovascular disease (CVD), non-CVD, and mortality risks of primary prevention individuals with very high coronary artery calcium (CAC; ≥1000), especially compared with rates observed in secondary prevention populations.
Methods: Our study population consisted of 6814 ethnically diverse individuals 45 to 84 years of age who were free of known CVD from MESA (Multi-Ethnic Study of Atherosclerosis), a prospective, observational, community-based cohort. Mean follow-up time was 13.6±4.4 years. Hazard ratios of CAC ≥1000 were compared with both CAC 0 and CAC 400 to 999 for CVD, non-CVD, and mortality outcomes with the use of Cox proportional hazards regression adjusted for age, sex, and traditional risk factors. Using a sex-adjusted logarithmic model, we calculated event rates in MESA as a function of CAC and compared them with those observed in the placebo group of stable secondary prevention patients in the FOURIER clinical trial (Further Cardiovascular Outcomes Research With PCSK9 Inhibition in Subjects With Elevated Risk).
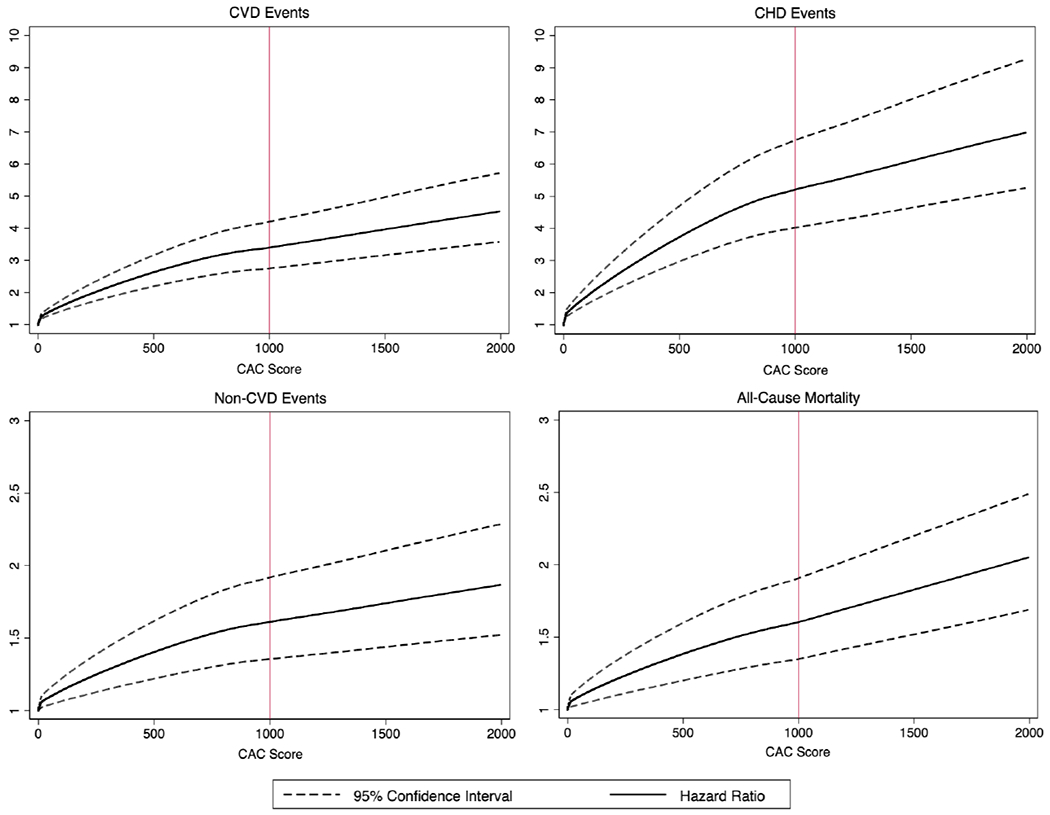
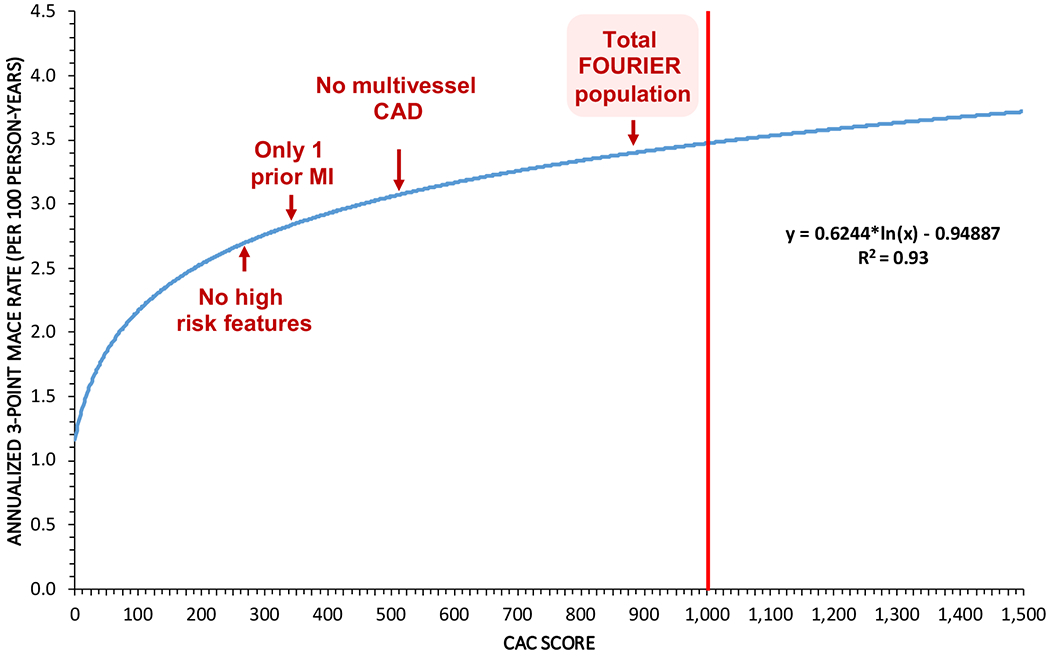
Results: Compared with CAC 400 to 999, those with CAC ≥1000 (n=257) had a greater mean number of coronary vessels with CAC (3.4±0.5), greater total area of CAC (586.5±275.2 mm2), similar CAC density, and more extensive extracoronary calcification. After full adjustment, CAC ≥1000 demonstrated a 4.71- (3.63-6.11), 7.57- (5.50-10.42), 4.86-(3.32-7.11), and 1.94-fold (1.57-2.41) increased risk for all CVD events, all coronary heart disease events, hard coronary heart disease events, and all-cause mortality, respectively, compared with CAC 0 and a 1.65- (1.25-2.16), 1.66- (1.22-2.25), 1.51- (1.03-2.23), and 1.34-fold (1.05-1.71) increased risk compared with CAC 400 to 999. With increasing CAC, hazard ratios increased for all event types, with no apparent upper CAC threshold. CAC ≥1000 was associated with a 1.95- (1.57-2.41) and 1.43-fold (1.12-1.83) increased risk for a first non-CVD event compared with CAC 0 and CAC 400 to 999, respectively. CAC 1000 corresponded to an annualized 3-point major adverse cardiovascular event rate of 3.4 per 100 person-years, similar to that of the total FOURIER population (3.3) and higher than those of the lower-risk FOURIER subgroups.
Conclusions: Individuals with very high CAC (≥1000) are a unique population at substantially higher risk for CVD events, non-CVD outcomes, and mortality than those with lower CAC, with 3-point major adverse cardiovascular event rates similar to those of a stable treated secondary prevention population. Future guidelines should consider a less distinct stratification algorithm between primary and secondary prevention patients in guiding aggressive preventive pharmacotherapy.
Keywords: cardiac imaging techniques; cardiovascular diseases; mortality; primary prevention; risk assessment; secondary prevention.
Figures
Comment in
-
Response by Peng et al to Letter Regarding Article, "Very High Coronary Artery Calcium (≥1000) and Association With Cardiovascular Disease Events, Non-Cardiovascular Disease Outcomes, and Mortality: Results From MESA".Circulation. 2021 Oct 26;144(17):e275-e276. doi: 10.1161/CIRCULATIONAHA.121.056534. Epub 2021 Oct 25. Circulation. 2021. PMID: 34694890 Free PMC article. No abstract available.
-
Letter by Braillon Regarding Article, "Very High Coronary Artery Calcium (≥1000) and Association With Cardiovascular Disease Events, Non-Cardiovascular Disease Outcomes, and Mortality: Results From MESA".Circulation. 2021 Oct 26;144(17):e274. doi: 10.1161/CIRCULATIONAHA.121.055717. Epub 2021 Oct 25. Circulation. 2021. PMID: 34694895 No abstract available.
References
-
- Shaw LJ, Raggi P, Schisterman E, Berman DS, Callister TQ. Prognostic value of cardiac risk factors and coronary artery calcium screening for all-cause mortality. Radiology. 2003;228:826–833. - PubMed
-
- Jaruvongvanich V, Wirunsawanya K, Sanguankeo A, Upala S. Nonalcoholic fatty liver disease is associated with coronary artery calcification: A systematic review and meta-analysis. Dig Liver Dis. 2016;48:1410–1417. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- N01 HC095168/HL/NHLBI NIH HHS/United States
- 75N92020D00001/HL/NHLBI NIH HHS/United States
- N01 HC095167/HL/NHLBI NIH HHS/United States
- HHSN268201500003I/HL/NHLBI NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- N01 HC095166/HL/NHLBI NIH HHS/United States
- N01 HC095160/HL/NHLBI NIH HHS/United States
- 75N92020D00002/HL/NHLBI NIH HHS/United States
- HHSN268201500003C/HL/NHLBI NIH HHS/United States
- N01 HC095161/HL/NHLBI NIH HHS/United States
- 75N92020D00005/HL/NHLBI NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- 75N92020D00003/HL/NHLBI NIH HHS/United States
- UL1 TR001420/TR/NCATS NIH HHS/United States
- 75N92020D00004/HL/NHLBI NIH HHS/United States
- N01 HC095163/HL/NHLBI NIH HHS/United States
- 75N92020D00007/HL/NHLBI NIH HHS/United States
- N01 HC095162/HL/NHLBI NIH HHS/United States
- 75N92020D00006/HL/NHLBI NIH HHS/United States
- N01 HC095165/HL/NHLBI NIH HHS/United States
- N01 HC095164/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
