

Contrast-enhanced Mammography: State of the Art
- PMID: 33650905
- PMCID: PMC7997616
- DOI: 10.1148/radiol.2021201948
Contrast-enhanced Mammography: State of the Art
Abstract
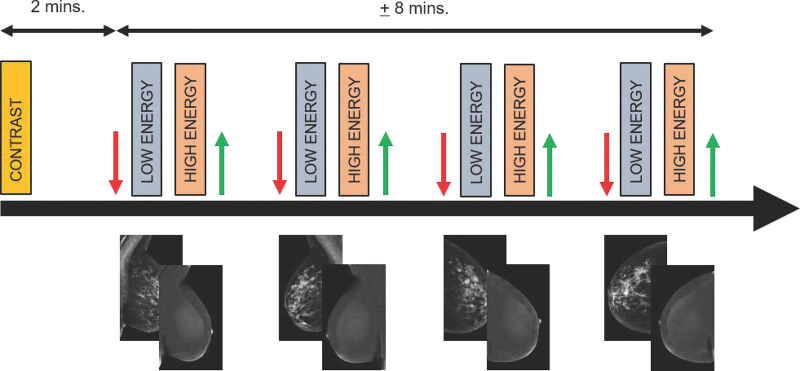
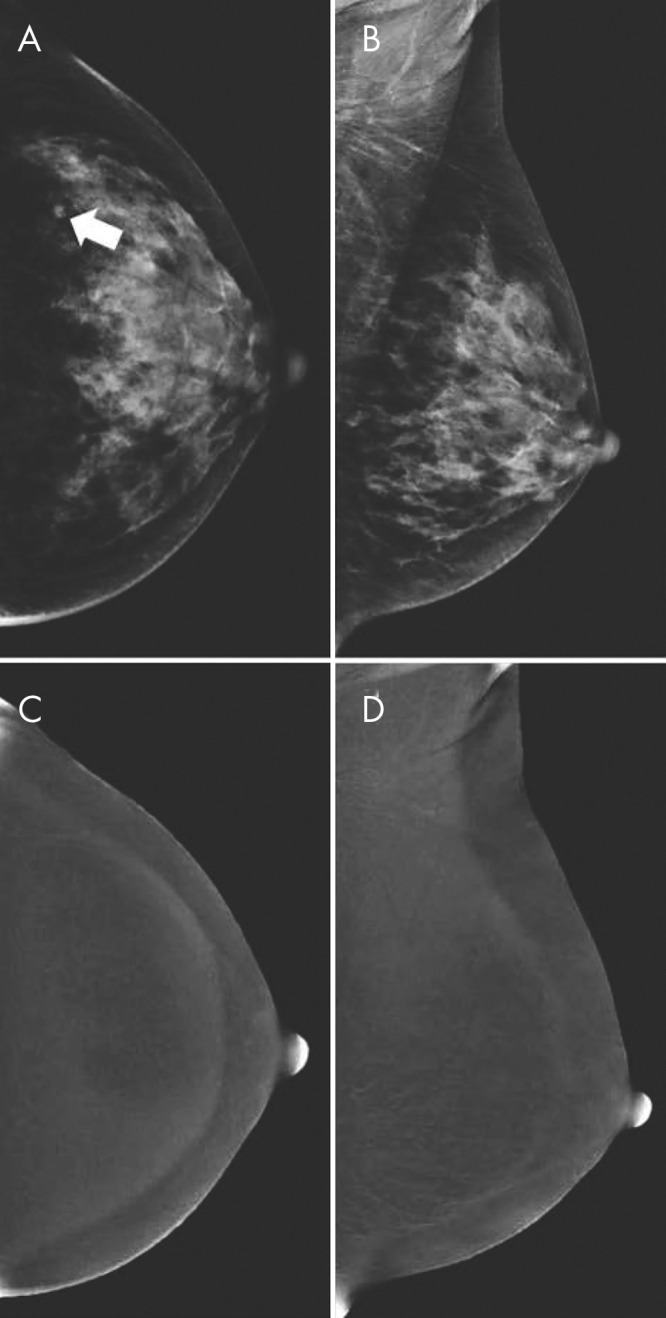
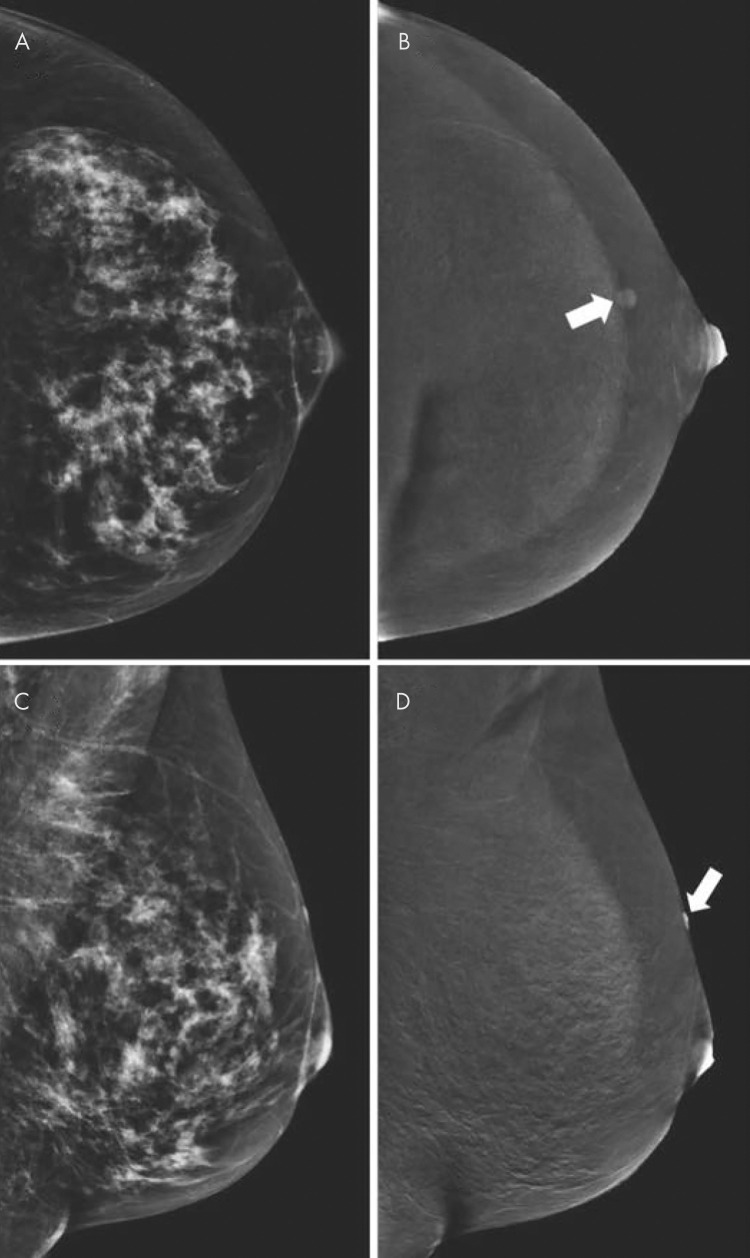
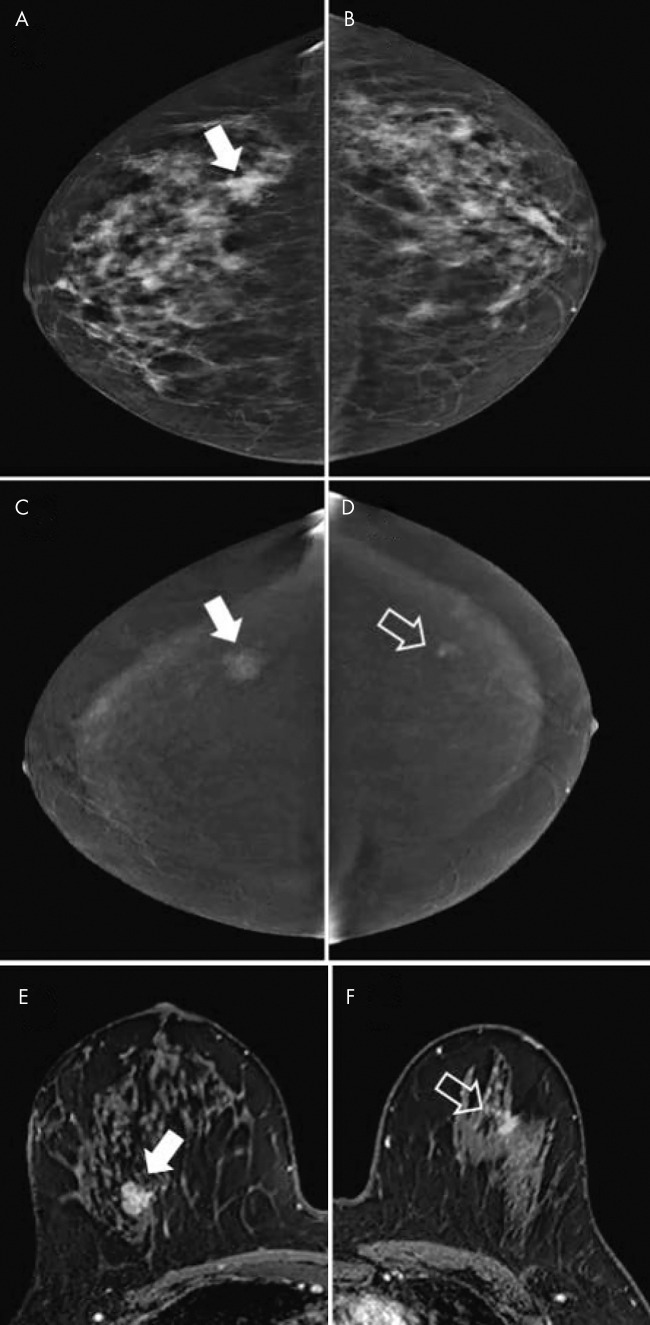
Contrast-enhanced mammography (CEM) has emerged as a viable alternative to contrast-enhanced breast MRI, and it may increase access to vascular imaging while reducing examination cost. Intravenous iodinated contrast materials are used in CEM to enhance the visualization of tumor neovascularity. After injection, imaging is performed with dual-energy digital mammography, which helps provide a low-energy image and a recombined or iodine image that depict enhancing lesions in the breast. CEM has been demonstrated to help improve accuracy compared with digital mammography and US in women with abnormal screening mammographic findings or symptoms of breast cancer. It has also been demonstrated to approach the accuracy of breast MRI in preoperative staging of patients with breast cancer and in monitoring response after neoadjuvant chemotherapy. There are early encouraging results from trials evaluating CEM in the screening of women who are at an increased risk of breast cancer. Although CEM is a promising tool, it slightly increases radiation dose and carries a small risk of adverse reactions to contrast materials. This review details the CEM technique, diagnostic and screening uses, and future applications, including artificial intelligence and radiomics.
© RSNA, 2021.
Figures


References
-
- Patel BK, Lobbes MBI, Lewin J. Contrast Enhanced Spectral Mammography: A Review. Semin Ultrasound CT MR 2018;39(1):70–79. - PubMed
-
- Kuhl C. The current status of breast MR imaging. Part I. Choice of technique, image interpretation, diagnostic accuracy, and transfer to clinical practice. Radiology 2007;244(2):356–378. - PubMed
-
- Carney PA, Miglioretti DL, Yankaskas BC, et al. Individual and combined effects of age, breast density, and hormone replacement therapy use on the accuracy of screening mammography. Ann Intern Med 2003;138(3):168–175. - PubMed
-
- Weigel S, Heindel W, Heidrich J, Hense HW, Heidinger O. Digital mammography screening: sensitivity of the programme dependent on breast density. Eur Radiol 2017;27(7):2744–2751. - PubMed
-
- Tagliafico AS, Calabrese M, Mariscotti G, et al. Adjunct Screening With Tomosynthesis or Ultrasound in Women With Mammography-Negative Dense Breasts: Interim Report of a Prospective Comparative Trial. J Clin Oncol 2016;34(16):1882–1888. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
