

Human-Computer Agreement of Electrocardiogram Interpretation for Patients Referred to and Declined for Primary Percutaneous Coronary Intervention: Retrospective Data Analysis Study
- PMID: 33650984
- PMCID: PMC7967222
- DOI: 10.2196/24188
Human-Computer Agreement of Electrocardiogram Interpretation for Patients Referred to and Declined for Primary Percutaneous Coronary Intervention: Retrospective Data Analysis Study
Abstract
Background: When a patient is suspected of having an acute myocardial infarction, they are accepted or declined for primary percutaneous coronary intervention partly based on clinical assessment of their 12-lead electrocardiogram (ECG) and ST-elevation myocardial infarction criteria.
Objective: We retrospectively determined the agreement rate between human (specialists called activator nurses) and computer interpretations of ECGs of patients who were declined for primary percutaneous coronary intervention.
Methods: Various features of patients who were referred for primary percutaneous coronary intervention were analyzed. Both the human and computer ECG interpretations were simplified to either "suggesting" or "not suggesting" acute myocardial infarction to avoid analysis of complex heterogeneous and synonymous diagnostic terms. Analyses, to measure agreement, and logistic regression, to determine if these ECG interpretations (and other variables such as patient age, chest pain) could predict patient mortality, were carried out.
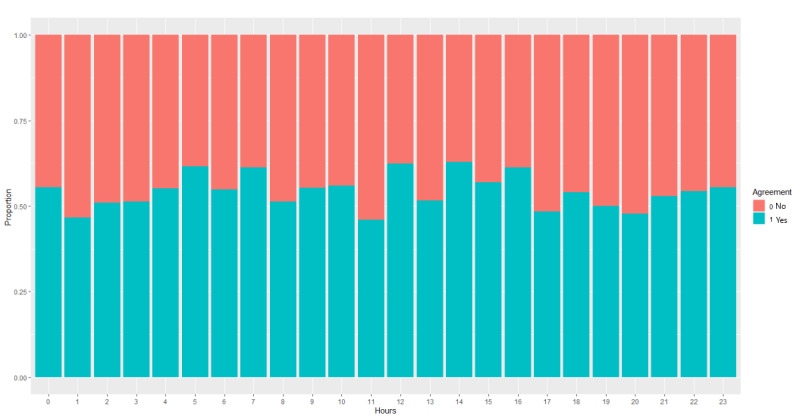
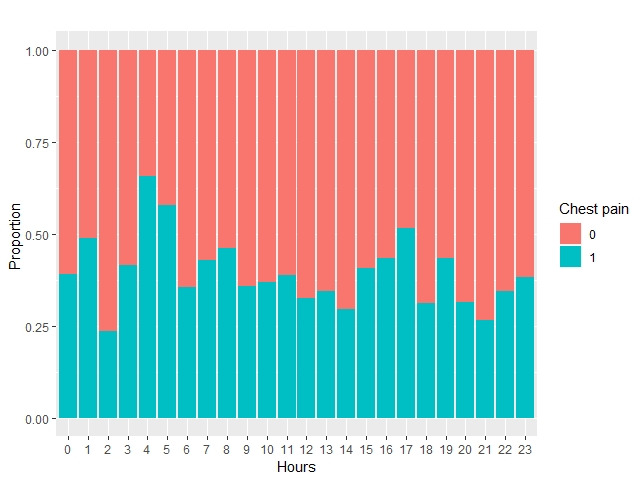
Results: Of a total of 1464 patients referred to and declined for primary percutaneous coronary intervention, 722 (49.3%) computer diagnoses suggested acute myocardial infarction, whereas 634 (43.3%) of the human interpretations suggested acute myocardial infarction (P<.001). The human and computer agreed that there was a possible acute myocardial infarction for 342 out of 1464 (23.3%) patients. However, there was a higher rate of human-computer agreement for patients not having acute myocardial infarctions (450/1464, 30.7%). The overall agreement rate was 54.1% (792/1464). Cohen κ showed poor agreement (κ=0.08, P=.001). Only the age (odds ratio [OR] 1.07, 95% CI 1.05-1.09) and chest pain (OR 0.59, 95% CI 0.39-0.89) independent variables were statistically significant (P=.008) in predicting mortality after 30 days and 1 year. The odds for mortality within 1 year of referral were lower in patients with chest pain compared to those patients without chest pain. A referral being out of hours was a trending variable (OR 1.41, 95% CI 0.95-2.11, P=.09) for predicting the odds of 1-year mortality.
Conclusions: Mortality in patients who were declined for primary percutaneous coronary intervention was higher than the reported mortality for ST-elevation myocardial infarction patients at 1 year. Agreement between computerized and human ECG interpretation is poor, perhaps leading to a high rate of inappropriate referrals. Work is needed to improve computer and human decision making when reading ECGs to ensure that patients are referred to the correct treatment facility for time-critical therapy.
Keywords: ECG interpretation; acute myocardial infarction; agreement between human and computer; diagnostic; electrocardiogram; heart; human-computer; infarction; intervention; primary percutaneous coronary intervention service; scan.
©Aleeha Iftikhar, Raymond Bond, Victoria Mcgilligan, Stephen J Leslie, Charles Knoery, James Shand, Adesh Ramsewak, Divyesh Sharma, Anne McShane, Khaled Rjoob, Aaron Peace. Originally published in JMIR Medical Informatics (http://medinform.jmir.org), 02.03.2021.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures


Similar articles
-
SPICED-ACS: Study of the potential impact of a computer-generated ECG diagnostic algorithmic certainty index in STEMI diagnosis: Towards transparent AI.J Electrocardiol. 2019 Nov-Dec;57S:S86-S91. doi: 10.1016/j.jelectrocard.2019.08.006. Epub 2019 Aug 13. J Electrocardiol. 2019. PMID: 31472927
-
Smoker's Paradox in Patients With ST-Segment Elevation Myocardial Infarction Undergoing Primary Percutaneous Coronary Intervention.J Am Heart Assoc. 2016 Apr 22;5(4):e003370. doi: 10.1161/JAHA.116.003370. J Am Heart Assoc. 2016. PMID: 27107131 Free PMC article.
-
The transtelephonic electrocardiogram-based triage is an independent predictor of decreased hospital mortality in patients with ST-segment elevation myocardial infarction treated with primary percutaneous coronary intervention.J Telemed Telecare. 2020 May;26(4):216-222. doi: 10.1177/1357633X18814335. Epub 2018 Dec 10. J Telemed Telecare. 2020. PMID: 30526257 Free PMC article.
-
Staged Percutaneous Intervention for Concurrent Chronic Total Occlusions in Patients With ST-Segment-Elevation Myocardial Infarction: A Systematic Review and Meta-Analysis.J Am Heart Assoc. 2018 Apr 13;7(8):e008415. doi: 10.1161/JAHA.117.008415. J Am Heart Assoc. 2018. PMID: 29654206 Free PMC article.
-
Efficacy and safety of thrombus aspiration in ST-segment elevation myocardial infarction: an updated systematic review and meta-analysis of randomised clinical trials.Eur Heart J Acute Cardiovasc Care. 2019 Feb;8(1):24-38. doi: 10.1177/2048872618795512. Epub 2018 Aug 30. Eur Heart J Acute Cardiovasc Care. 2019. PMID: 30160519
References
-
- Heart statistics. British Heart Foundation. [2020-05-01]. https://www.bhf.org.uk/what-we-do/our-research/heart-statistics.
-
- Amsterdam EA, Wenger NK, Brindis RG, Casey DE, Ganiats TG, Holmes DR, Jaffe AS, Jneid H, Kelly RF, Kontos MC, Levine GN, Liebson PR, Mukherjee D, Peterson ED, Sabatine MA, Smalling RW, Zieman SJ, ACC/AHA Task Force Members 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014 Dec 23;130(25):e344–426. doi: 10.1161/CIR.0000000000000134. - DOI - PubMed
-
- Diagnosis-heart attack. UK National Health Service. [2020-04-02]. https://www.nhs.uk/conditions/heart-attack/diagnosis/
LinkOut - more resources
Full Text Sources
Other Literature Sources
