

Integrated Polygenic Tool Substantially Enhances Coronary Artery Disease Prediction
- PMID: 33651632
- PMCID: PMC8284388
- DOI: 10.1161/CIRCGEN.120.003304
Integrated Polygenic Tool Substantially Enhances Coronary Artery Disease Prediction
Erratum in
-
Correction to: Integrated Polygenic Tool Substantially Enhances Coronary Artery Disease Prediction.Circ Genom Precis Med. 2021 Aug;14(4):e000085. doi: 10.1161/HCG.0000000000000085. Epub 2021 Aug 17. Circ Genom Precis Med. 2021. PMID: 34403262 Free PMC article. No abstract available.
Abstract
Background: There is considerable interest in whether genetic data can be used to improve standard cardiovascular disease risk calculators, as the latter are routinely used in clinical practice to manage preventative treatment.
Methods: Using the UK Biobank resource, we developed our own polygenic risk score for coronary artery disease (CAD). We used an additional 60 000 UK Biobank individuals to develop an integrated risk tool (IRT) that combined our polygenic risk score with established risk tools (either the American Heart Association/American College of Cardiology pooled cohort equations [PCE] or UK QRISK3), and we tested our IRT in an additional, independent set of 186 451 UK Biobank individuals.
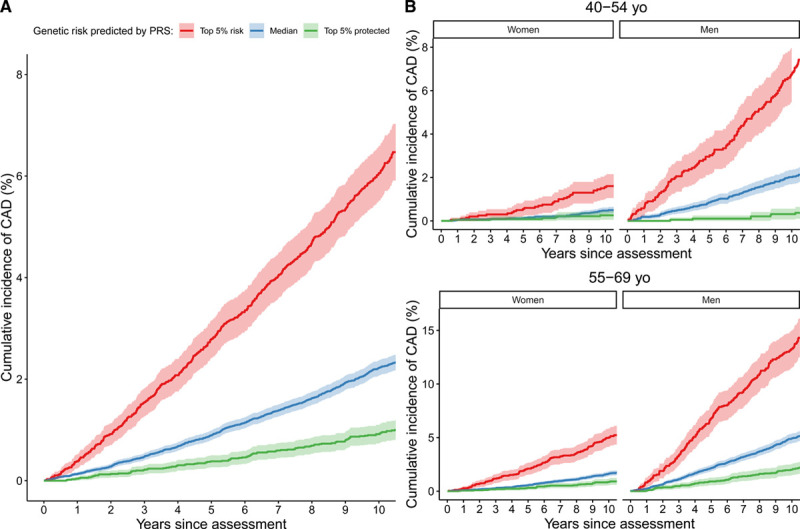
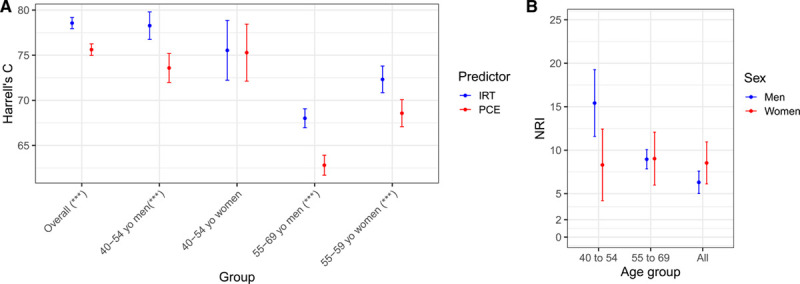
Results: The novel CAD polygenic risk score shows superior predictive power for CAD events, compared with other published polygenic risk scores, and is largely uncorrelated with PCE and QRISK3. When combined with PCE into an IRT, it has superior predictive accuracy. Overall, 10.4% of incident CAD cases were misclassified as low risk by PCE and correctly classified as high risk by the IRT, compared with 4.4% misclassified by the IRT and correctly classified by PCE. The overall net reclassification improvement for the IRT was 5.9% (95% CI, 4.7-7.0). When individuals were stratified into age-by-sex subgroups, the improvement was larger for all subgroups (range, 8.3%-15.4%), with the best performance in 40- to 54-year-old men (15.4% [95% CI, 11.6-19.3]). Comparable results were found using a different risk tool (QRISK3) and also a broader definition of cardiovascular disease. Use of the IRT is estimated to avoid up to 12 000 deaths in the United States over a 5-year period.
Conclusions: An IRT that includes polygenic risk outperforms current risk stratification tools and offers greater opportunity for early interventions. Given the plummeting costs of genetic tests, future iterations of CAD risk tools would be enhanced with the addition of a person's polygenic risk.
Keywords: coronary artery disease; genetic epidemiology; genetics; primary prevention; risk factors.
Figures

References
-
- Roth GA, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, Abbastabar H, Abd-Allah F, Abdela J, Abdelalim A, et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018; 392:1736–1788 - PMC - PubMed
-
- Califf RM, Armstrong PW, Carver JR, D’Agostino RB, Strauss WE. 27th Bethesda Conference: matching the intensity of risk factor management with the hazard for coronary disease events. Task Force 5. Stratification of patients into high, medium and low risk subgroups for purposes of risk factor management. J Am Coll Cardiol. 1996; 27:1007–1019. doi: 10.1016/0735-1097(96)87733-3 - PubMed
-
- Goff DC, Jr, Lloyd-Jones DM, Bennett G, Coady S, D’Agostino RB, Gibbons R, Greenland P, Lackland DT, Levy D, O’Donnell CJ, et al. ; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014; 129(25 suppl 2):S49–S73. doi: 10.1161/01.cir.0000437741.48606.98 - PubMed
-
- Arnett DK, Blumenthal RS, Albert MA, Buroker AB, Goldberger ZD, Hahn EJ, Himmelfarb CD, Khera A, Lloyd-Jones D, McEvoy JW, et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2019; 74:e177–e232. doi: 10.1016/j.jacc.2019.03.010 - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
