

Melanoma brain metastasis presentation, treatment, and outcomes in the age of targeted and immunotherapies
- PMID: 33651913
- PMCID: PMC9275782
- DOI: 10.1002/cncr.33459
Melanoma brain metastasis presentation, treatment, and outcomes in the age of targeted and immunotherapies
Abstract
Background: Historically, the prognosis for patients who have melanoma brain metastasis (MBM) has been dismal. However, breakthroughs in targeted and immunotherapies have improved long-term survival in those with advanced melanoma. Therefore, MBM presentation, prognosis, and the use of multimodality central nervous system (CNS)-directed treatment were reassessed.
Methods: In this retrospective study, the authors evaluated patients with MBM who received treatment at Memorial Sloan Kettering Cancer Center between 2010 and 2019. Kaplan-Meier methodology was used to describe overall survival (OS). Recursive partitioning analysis and time-dependent multivariable Cox modeling were used to assess prognostic variables and to associate CNS-directed treatments with OS.
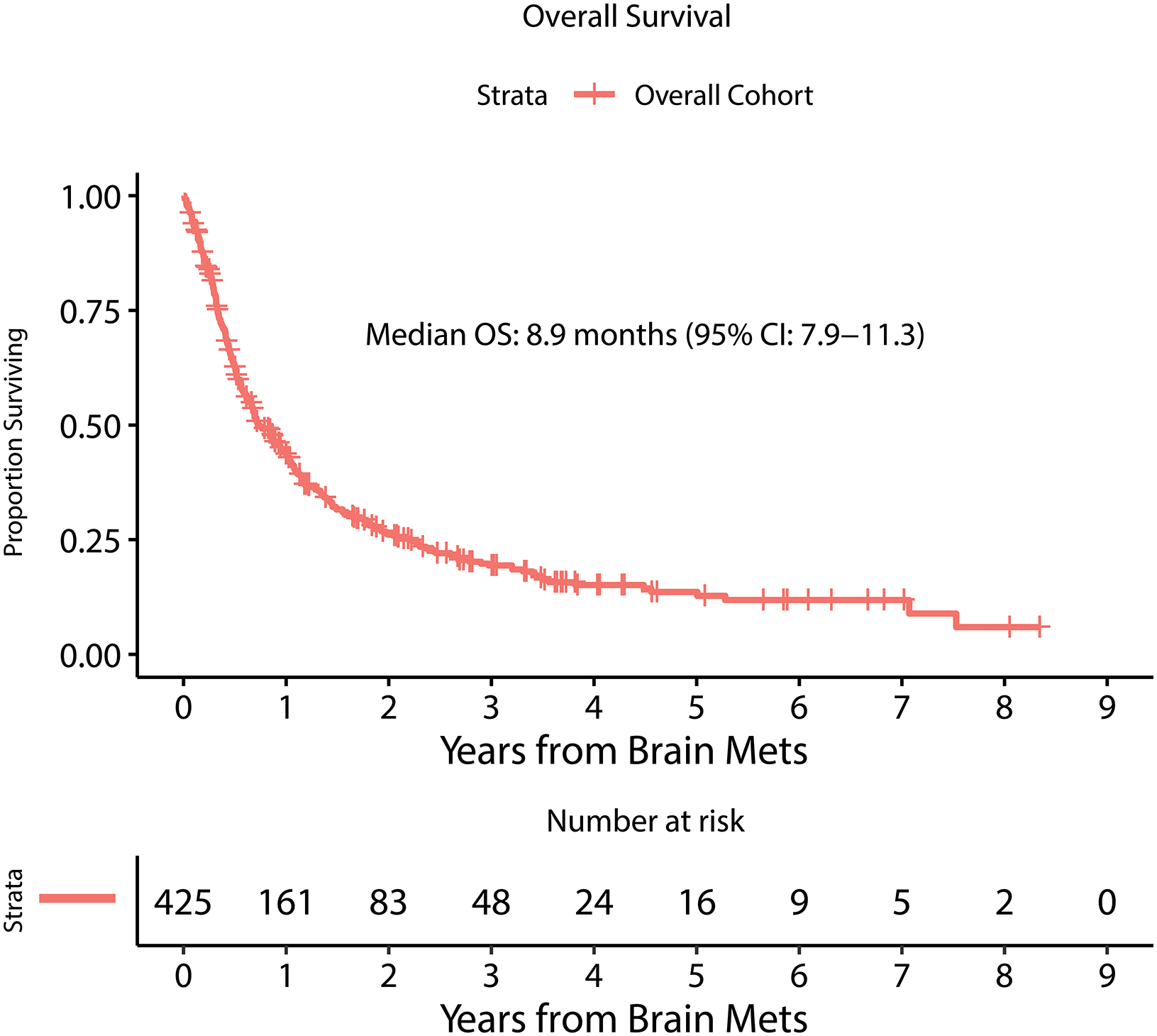
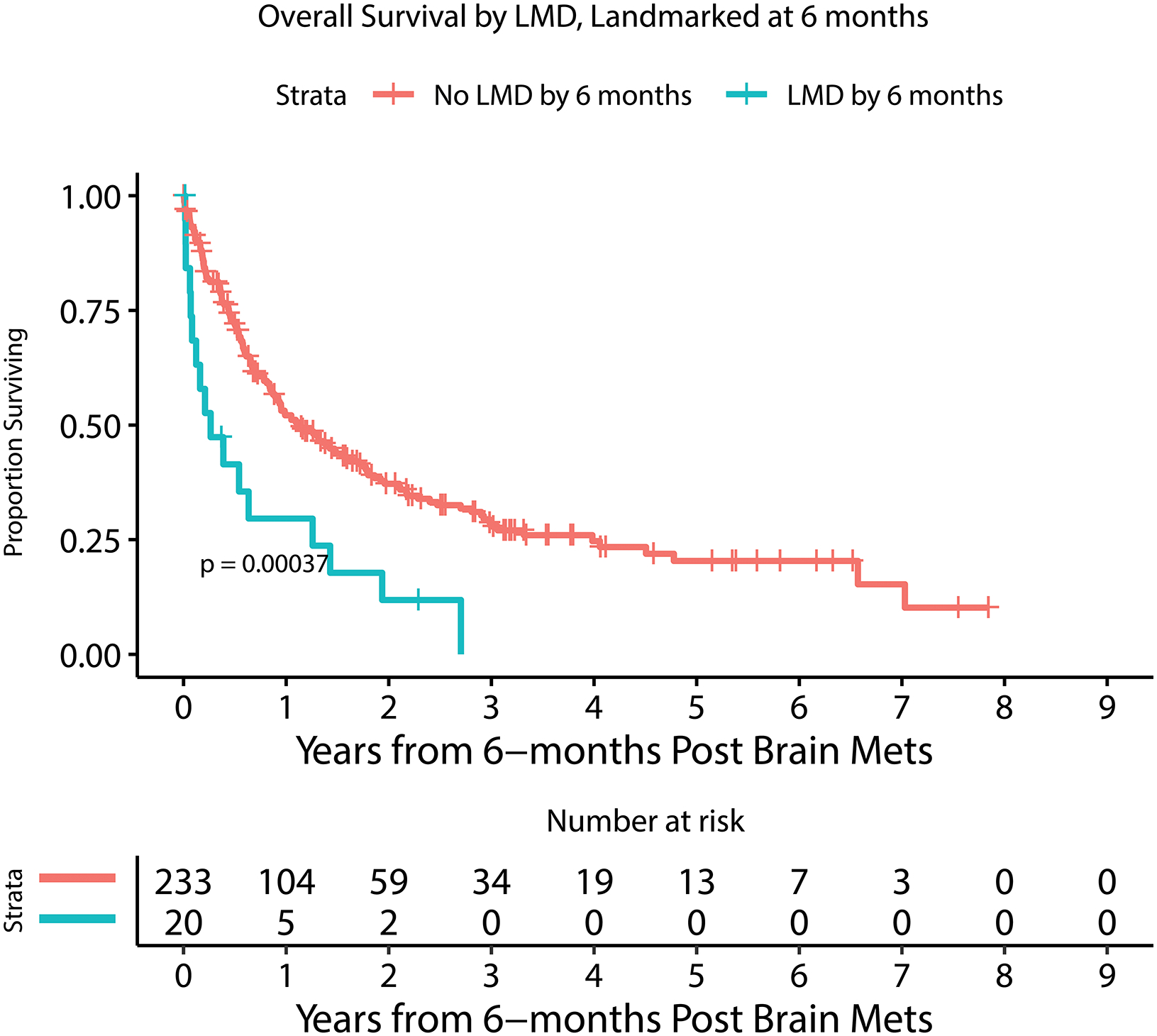
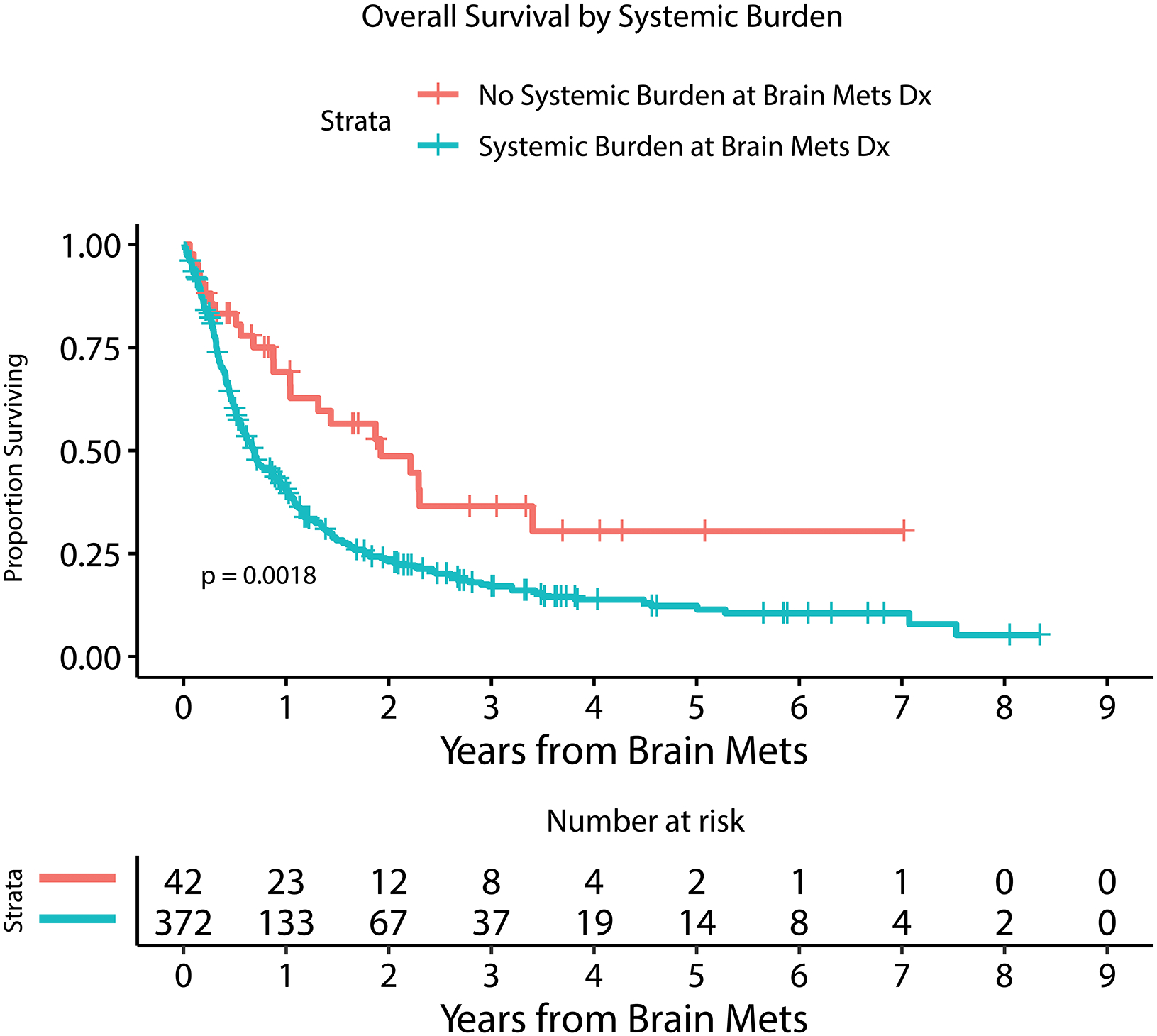
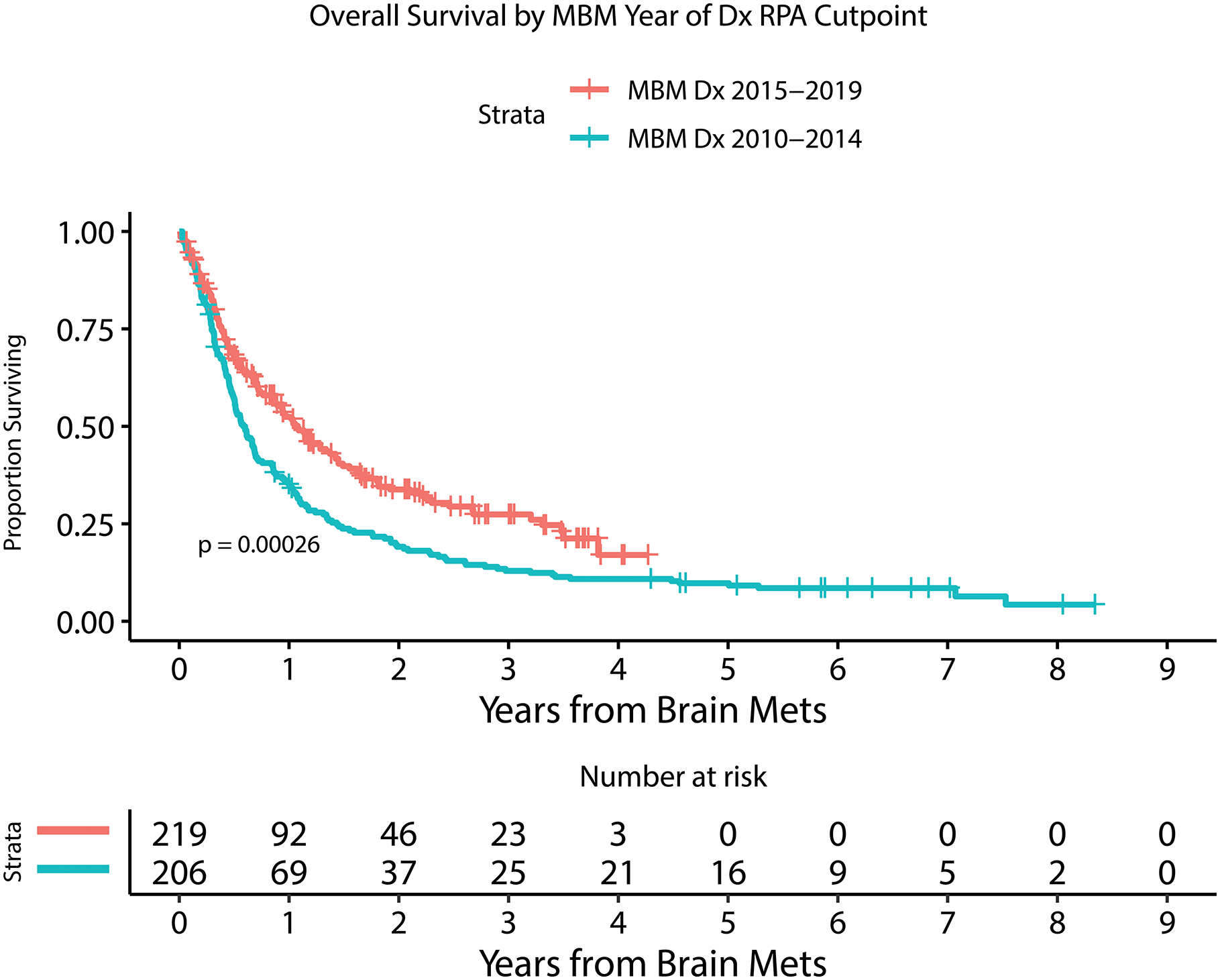
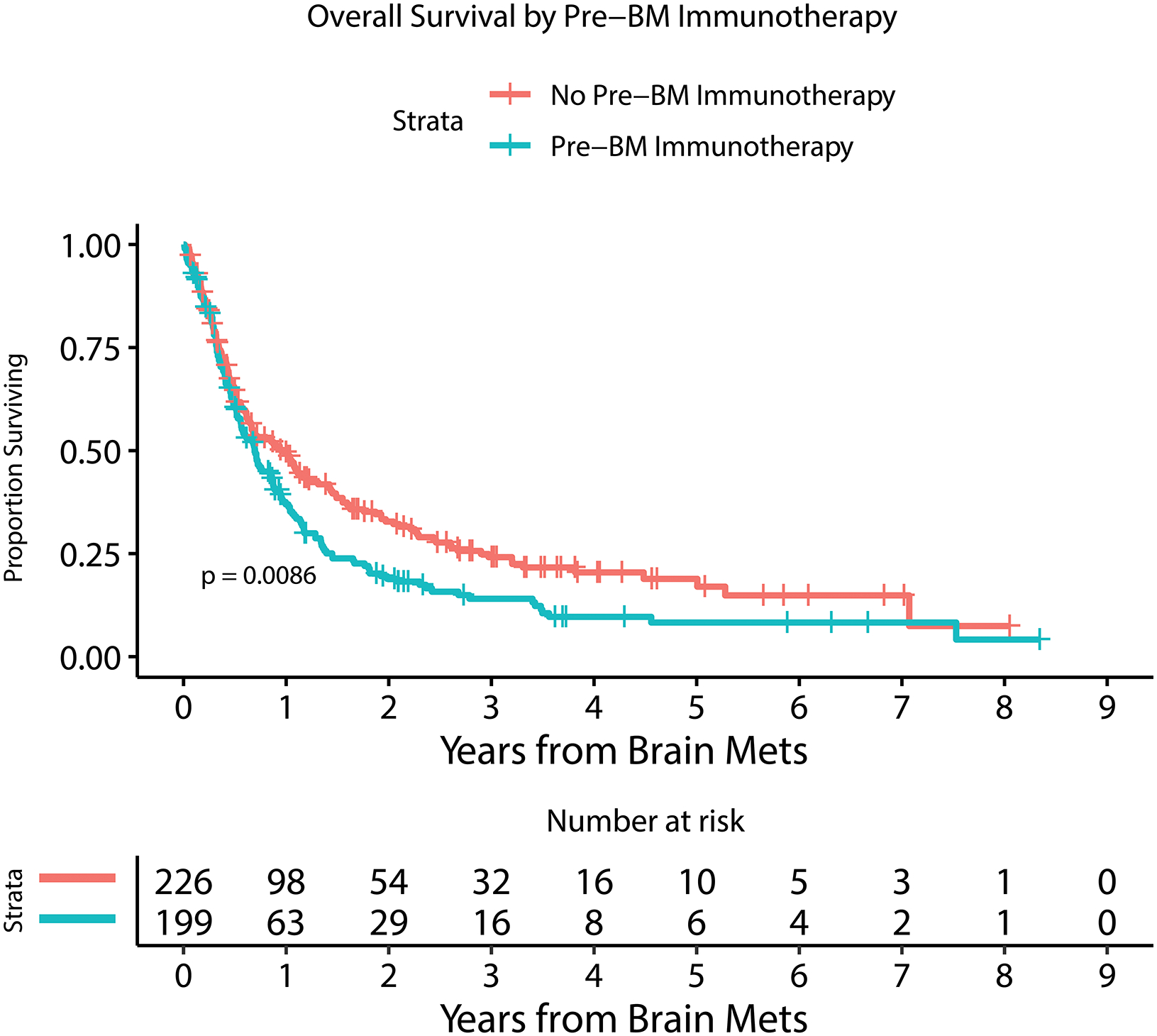
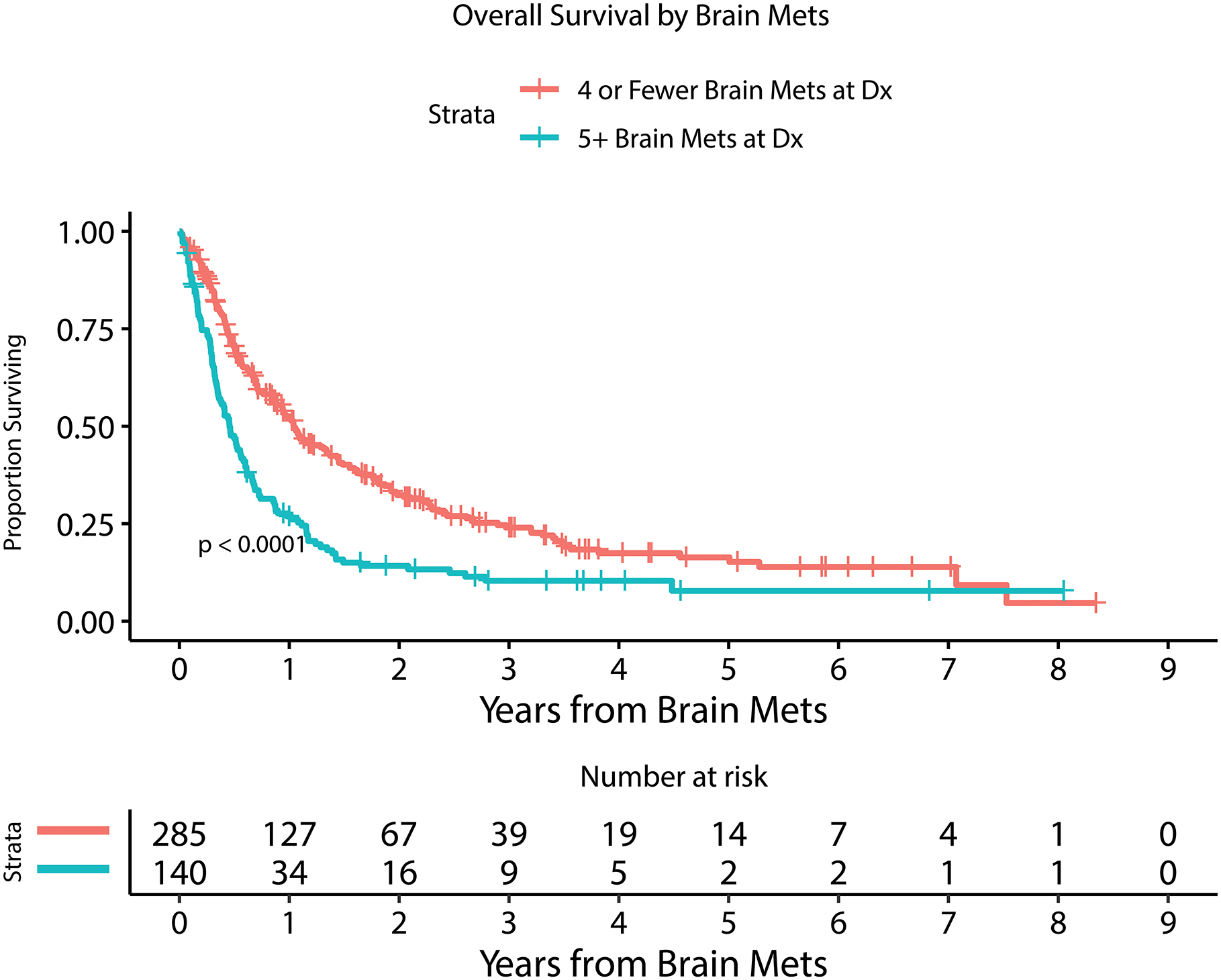
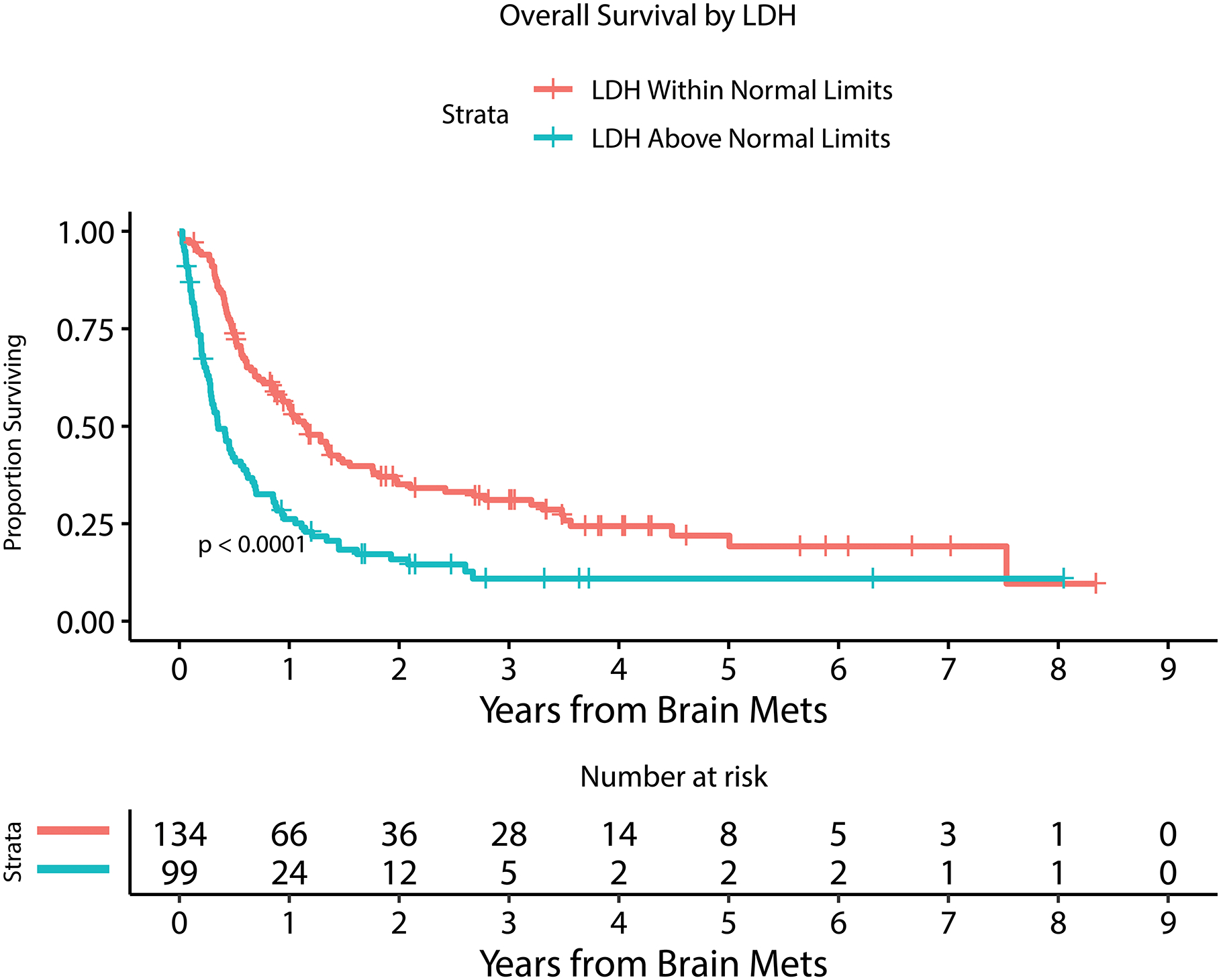
Results: Four hundred twenty-five patients with 2488 brain metastases were included. The median OS after an MBM diagnosis was 8.9 months (95% CI, 7.9-11.3 months). Patients who were diagnosed with MBM between 2015 and 2019 experienced longer OS compared to those who were diagnosed between 2010 and 2014 (OS, 13.0 months [95% CI, 10.47-17.06 months] vs 7.0 months [95% CI, 6.1-8.3 months]; P = .0003). Prognostic multivariable modeling significantly associated shortened OS independently with leptomeningeal dissemination (P < .0001), increasing numbers of brain metastases at diagnosis (P < .0001), earlier MBM diagnosis year (P = .0008), higher serum levels of lactate dehydrogenase (P < .0001), receipt of immunotherapy before MBM diagnosis (P = .003), and the presence of extracranial disease (P = .02). The use of different CNS-directed treatment modalities was associated with presenting symptoms, diagnosis year, number and size of brain metastases, and the presence of extracranial disease. Multivariable analysis demonstrated improved survival for patients who underwent craniotomy (P = .01).
Conclusions: The prognosis for patients with MBM has improved within the last 5 years, coinciding with the approval of PD-1 immune checkpoint blockade and combined BRAF/MEK targeting. Improving survival reflects and may influence the willingness to use aggressive multimodality treatment for MBM.
Lay summary: Historically, melanoma brain metastases (MBM) have carried a poor survival prognosis of 4 to 6 months; however, the introduction of immunotherapy and targeted precision medicines has altered the survival curve for advanced melanoma. In this large, single-institution, contemporary cohort, the authors demonstrate a significant increase in survival of patients with MBM to 13 months within the last 5 years of the study. A worse prognosis for patients with MBM was significantly associated with the number of metastases at diagnosis, previous exposure to immunotherapy, spread of disease to the leptomeningeal compartment, serum lactate dehydrogenase elevation, and the presence of extracranial disease. The current age of systemic treatments has also been accompanied by shifts in the use of central nervous system-directed therapies.
Keywords: brain metastases; immunotherapy; melanoma; survival; targeted therapy.
© 2021 American Cancer Society.
Figures
References
-
- Barnholtz-Sloan JS, Sloan AE, Davis FG, Vigneau FD, Lai P, Sawaya RE. Incidence proportions of brain metastases in patients diagnosed (1973 to 2001) in the Metropolitan Detroit Cancer Surveillance System. J Clin Oncol Off J Am Soc Clin Oncol. 2004;22(14):2865–2872. doi: 10.1200/JCO.2004.12.149 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
