

Alternative Flicker Glass: A New Anti-Suppression Approach to the Treatment of Anisometropic Amblyopia
- PMID: 33652438
- PMCID: PMC8743914
- DOI: 10.1159/000515599
Alternative Flicker Glass: A New Anti-Suppression Approach to the Treatment of Anisometropic Amblyopia
Abstract
Introduction: Amblyopia always presents with monocular and binocular dysfunction. In this study, we aim to investigate the efficacy of alternative occlusion using liquid crystal glasses versus continuous occlusion therapy using traditional patches for treating amblyopia.
Methods: Eligible subjects with anisometropic amblyopia were randomized into 2 groups: alternative flicker glass (AFG) or patching group. In the AFG group, subjects were instructed to wear the flicker glasses for 1 h a day. The AFG is a lightweight spectacle frame with liquid crystal lenses that provide direct square-wave alternating occlusion, which were preprogrammed at a temporal frequency of 7 Hz. In the patching group, the patients were prescribed to wear traditional patches for 2 h a day. The best-corrected visual acuity (BCVA), contrast sensitivity function (CSF), and stereoacuity were measured at the baseline and 3 and 12 weeks.
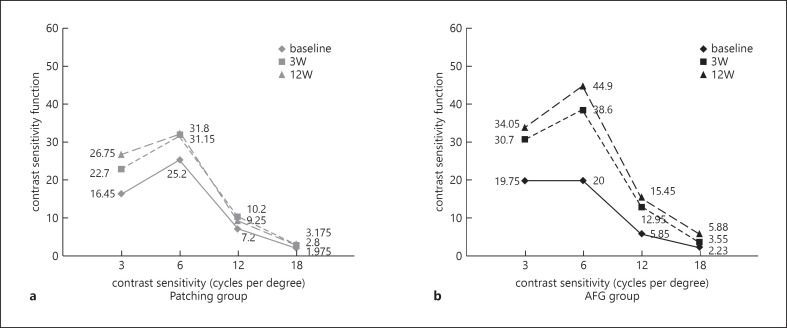
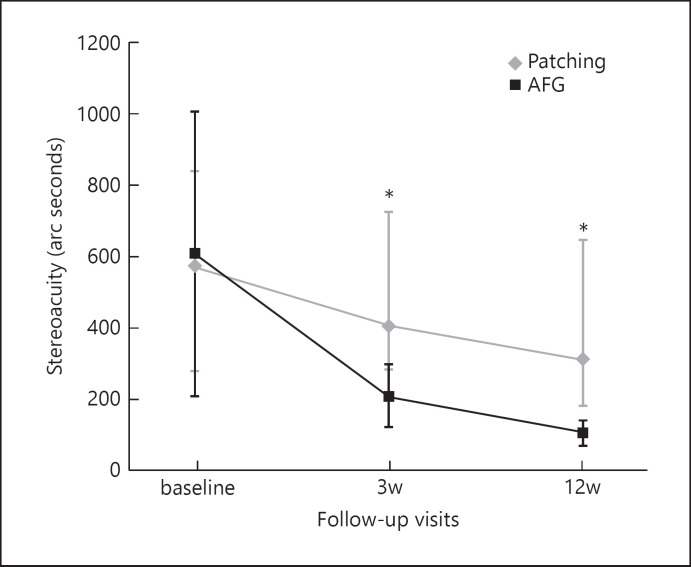
Results: In this pilot study, a total of 40 children were recruited, with 20 in the AFG group. Mean BCVA improved by 0.17 ± 0.14 logMAR (95% CI = 0.10-0.23) in the AFG group and 0.18 ± 0.18 logMAR (95% CI = 0.09-0.26) in the patching group from baseline to 12 weeks. The improvement in BCVA in both groups was significant (both p < 0.01), while there was no significant difference between the groups (p = 0.82). The CSF of both low and high spatial frequencies exhibited significant improvement at 12 weeks in the AFG group (p < 0.01, respectively) and just had a significant improvement at low spatial frequency in the patching group (p < 0.01). The stereoacuity significantly improved by 504.00 ± 848.00 (95% CI = 107.12 to 900.88) arc seconds in the AFG group (p < 0.05), while it was 263.50 ± 639.55 (95% CI = -35.82 to 562.82) arc seconds in the patching group (p > 0.05).
Conclusion: Alternative flicker glass was effective in improving both monocular and binocular function, which was most likely achieved by reducing suppression and promoting binocular fusion. This therapy exhibited promise as an alternative method for amblyopia treatment.
Keywords: Alternative flicker glass; Anisometropic amblyopia; Contrast sensitivity; Stereoacuity.
© 2021 The Author(s). Published by S. Karger AG, Basel.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures


References
-
- Huang C, Tao L, Zhou Y, Lu ZL. Treated amblyopes remain deficient in spatial vision: a contrast sensitivity and external noise study. Vision Res. 2007 Jan;47((1)):22–34. - PubMed
-
- Bhola R, Keech RV, Kutschke P, Pfeifer W, Scott WE. Recurrence of amblyopia after occlusion therapy. Ophthalmology. 2006 Nov;113((11)):2097–100. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
