

Central Nervous System Mold Infections in Children with Hematological Malignancies: Advances in Diagnosis and Treatment
- PMID: 33652605
- PMCID: PMC7996787
- DOI: 10.3390/jof7030168
Central Nervous System Mold Infections in Children with Hematological Malignancies: Advances in Diagnosis and Treatment
Abstract
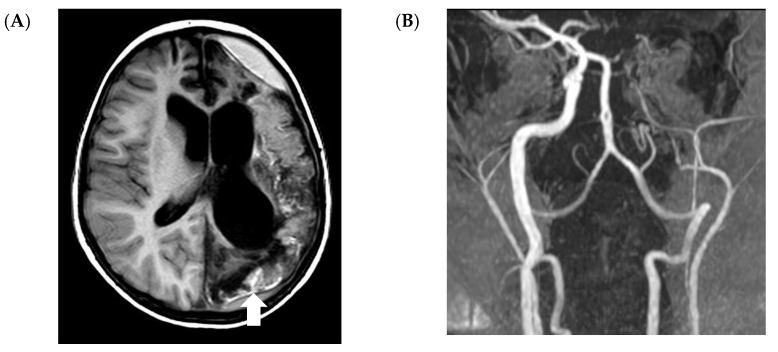
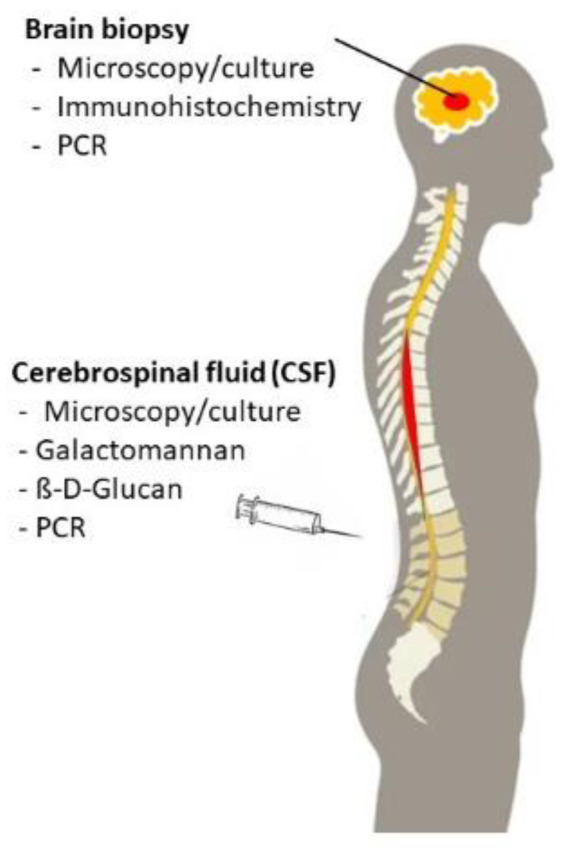
The incidence of invasive mold disease (IMD) has significantly increased over the last decades, and IMD of the central nervous system (CNS) is a particularly severe form of this infection. Solid data on the incidence of CNS IMD in the pediatric setting are lacking, in which Aspergillus spp. is the most prevalent pathogen, followed by mucorales. CNS IMD is difficult to diagnose, and although imaging tools such as magnetic resonance imaging have considerably improved, these techniques are still unspecific. As microscopy and culture have a low sensitivity, non-culture-based assays such as the detection of fungal antigens (e.g., galactomannan or beta-D-glucan) or the detection of fungal nucleic acids by molecular assays need to be validated in children with suspected CNS IMD. New and potent antifungal compounds helped to improve outcome of CNS IMD, but not all agents are approved for children and a pediatric dosage has not been established. Therefore, studies have to rapidly evaluate dosage, safety and efficacy of antifungal compounds in the pediatric setting. This review will summarize the current knowledge on diagnostic tools and on the management of CNS IMD with a focus on pediatric patients.
Keywords: Aspergillus; central nervous system; child; invasive fungal disease; mold; mucormycetes.
Conflict of interest statement
T.L. has a consultant relationship with Gilead Sciences, Merck/MSD, Mundipharma, Pfizer, Astellas, and Roche, serves at the speakers bureau of Gilead Sciences, Merck/MSD, Astellas, Pfizer, and GSK and received unrestricted research support from Gilead Sciences. All other authors do not have a conflict of interest relevant to this article to disclose.
Figures
Similar articles
-
Invasive mold disease of the central nervous system in children and adolescents with cancer or undergoing hematopoietic stem cell transplantation: Analysis of 29 contemporary patients.Pediatr Blood Cancer. 2019 Aug;66(8):e27806. doi: 10.1002/pbc.27806. Epub 2019 May 7. Pediatr Blood Cancer. 2019. PMID: 31066209
-
Galactomannan and PCR in the Central Nervous System to Detect Invasive Mold Disease - A Retrospective Analysis in Immunocompromised Children.Sci Rep. 2019 Sep 10;9(1):12950. doi: 10.1038/s41598-019-49426-0. Sci Rep. 2019. PMID: 31506548 Free PMC article.
-
Diagnosis of invasive mold diseases in patients with hematological malignancies using Aspergillus, Mucorales, and panfungal PCR in BAL.Transpl Infect Dis. 2018 Oct;20(5):e12953. doi: 10.1111/tid.12953. Epub 2018 Jun 28. Transpl Infect Dis. 2018. PMID: 29896857
-
An Update on the Diagnosis and Treatment of Invasive Mold Disease of the Central Nervous System in Children.Pediatr Infect Dis J. 2023 Apr 1;42(4):e119-e121. doi: 10.1097/INF.0000000000003780. Epub 2022 Nov 30. Pediatr Infect Dis J. 2023. PMID: 36730048 Review.
-
Diagnostic Approaches for Invasive Aspergillosis-Specific Considerations in the Pediatric Population.Front Microbiol. 2018 Mar 26;9:518. doi: 10.3389/fmicb.2018.00518. eCollection 2018. Front Microbiol. 2018. PMID: 29632518 Free PMC article. Review.
Cited by
-
Central Nervous System Fungal Diseases in Children with Malignancies: A 16-Year Study from the Infection Working Group of the Hellenic Society of Pediatric Hematology Oncology.J Fungi (Basel). 2024 Sep 14;10(9):654. doi: 10.3390/jof10090654. J Fungi (Basel). 2024. PMID: 39330414 Free PMC article.
-
Metagenomic next-generation sequencing could play a pivotal role in validating the diagnosis of invasive mold disease of the central nervous system.Front Cell Infect Microbiol. 2024 Jun 7;14:1393242. doi: 10.3389/fcimb.2024.1393242. eCollection 2024. Front Cell Infect Microbiol. 2024. PMID: 38912204 Free PMC article.
-
Hyphal penetration is the major pathway of translocation of Candida albicans across the blood-cerebrospinal fluid barrier.Fluids Barriers CNS. 2025 Apr 4;22(1):34. doi: 10.1186/s12987-025-00644-x. Fluids Barriers CNS. 2025. PMID: 40181464 Free PMC article.
-
Development of a Monoclonal Antibody and a Serodiagnostic Lateral-Flow Device Specific to Rhizopus arrhizus (Syn. R. oryzae), the Principal Global Agent of Mucormycosis in Humans.J Fungi (Basel). 2022 Jul 21;8(7):756. doi: 10.3390/jof8070756. J Fungi (Basel). 2022. PMID: 35887511 Free PMC article.
-
Invasive Fungal Infections in Children with Haematological Malignancies: Diagnostic and Therapeutic Challenges.J Fungi (Basel). 2021 Jun 28;7(7):516. doi: 10.3390/jof7070516. J Fungi (Basel). 2021. PMID: 34203146 Free PMC article.
References
-
- Cesaro S., Tridello G., Castagnola E., Calore E., Carraro F., Mariotti I., Colombini A., Perruccio K., Decembrino N., Russo G., et al. Retrospective study on the incidence and outcome of proven and probable invasive fungal infections in high-risk pediatric onco-hematological patients. Eur. J. Haematol. 2017;99:240–248. doi: 10.1111/ejh.12910. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
