

Concomitant surgical ablation for atrial fibrillation is associated with increased risk of acute kidney injury but improved late survival
- PMID: 33653608
- PMCID: PMC8608247
- DOI: 10.1016/j.jtcvs.2021.01.023
Concomitant surgical ablation for atrial fibrillation is associated with increased risk of acute kidney injury but improved late survival
Abstract
Background: Acute kidney injury (AKI) after cardiac surgery remains a common complication that has been associated with increased morbidity and mortality. This study implemented Kidney Disease Improving Global Outcomes criteria to evaluate renal outcomes after concomitant surgical ablation for atrial fibrillation.
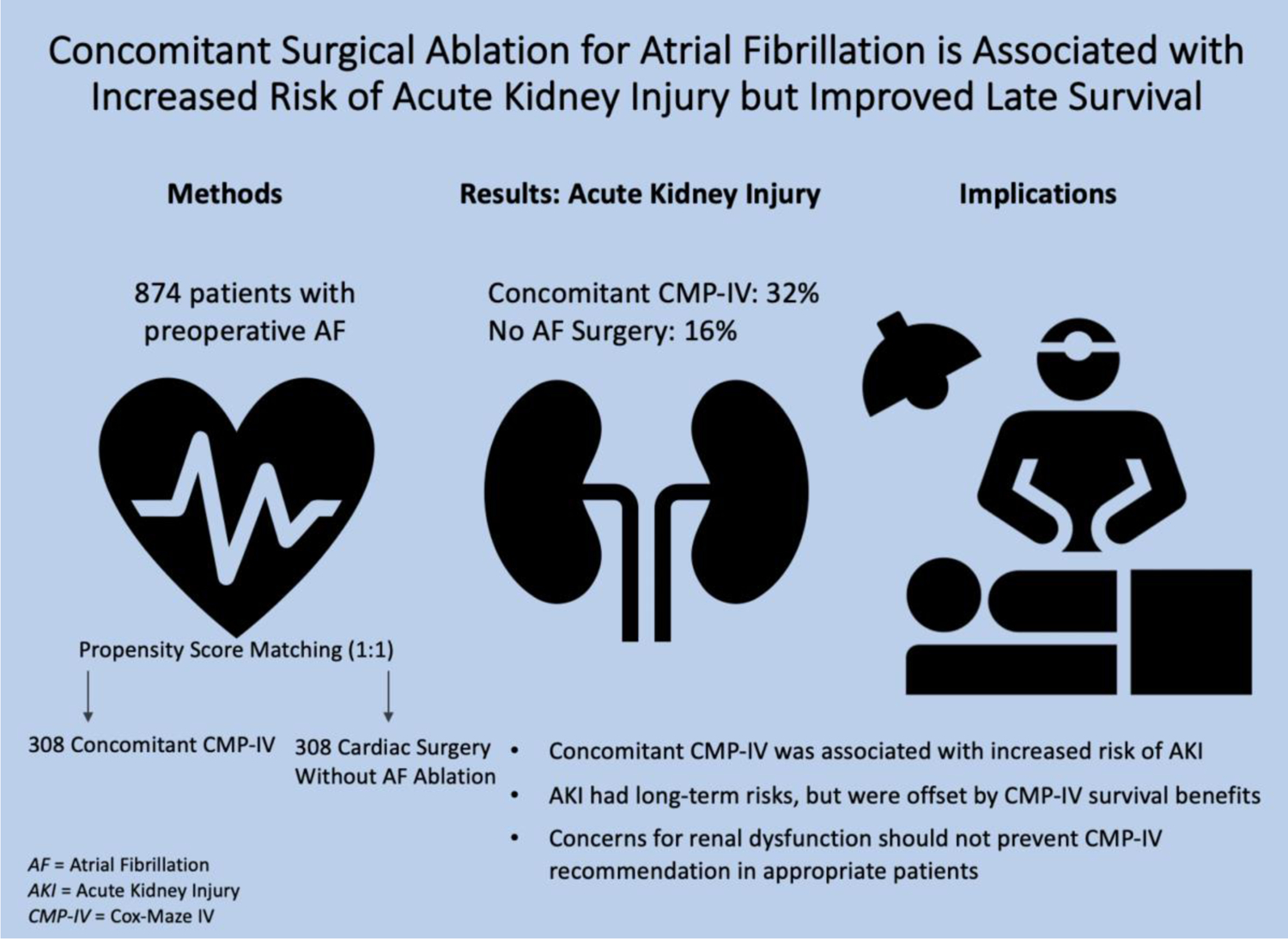
Methods: Patients with a history of atrial fibrillation who underwent elective cardiac surgery at our institution from 2008 to 2018 were retrospectively reviewed. Those with preoperative renal dysfunction were excluded. Patients were classified as those who underwent concomitant Cox-Maze IV (CMP-IV) (n = 376) or no surgical ablation (n = 498). Nearest neighbor 1:1 propensity matching was conducted on fourteen covariates. AKI was evaluated by mixed effects logistic regression analysis. Long-term survival was evaluated by proportional hazards regression.
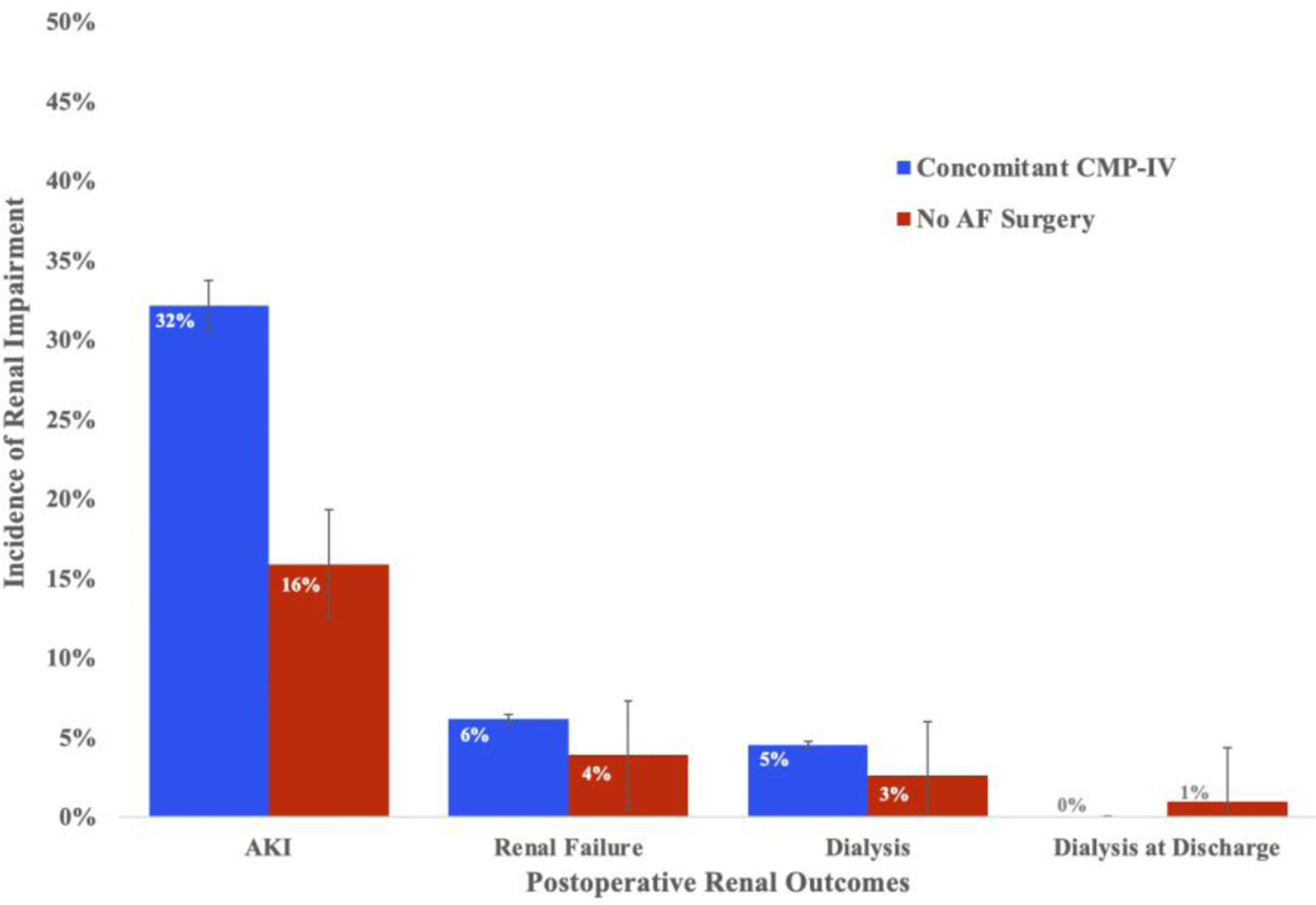
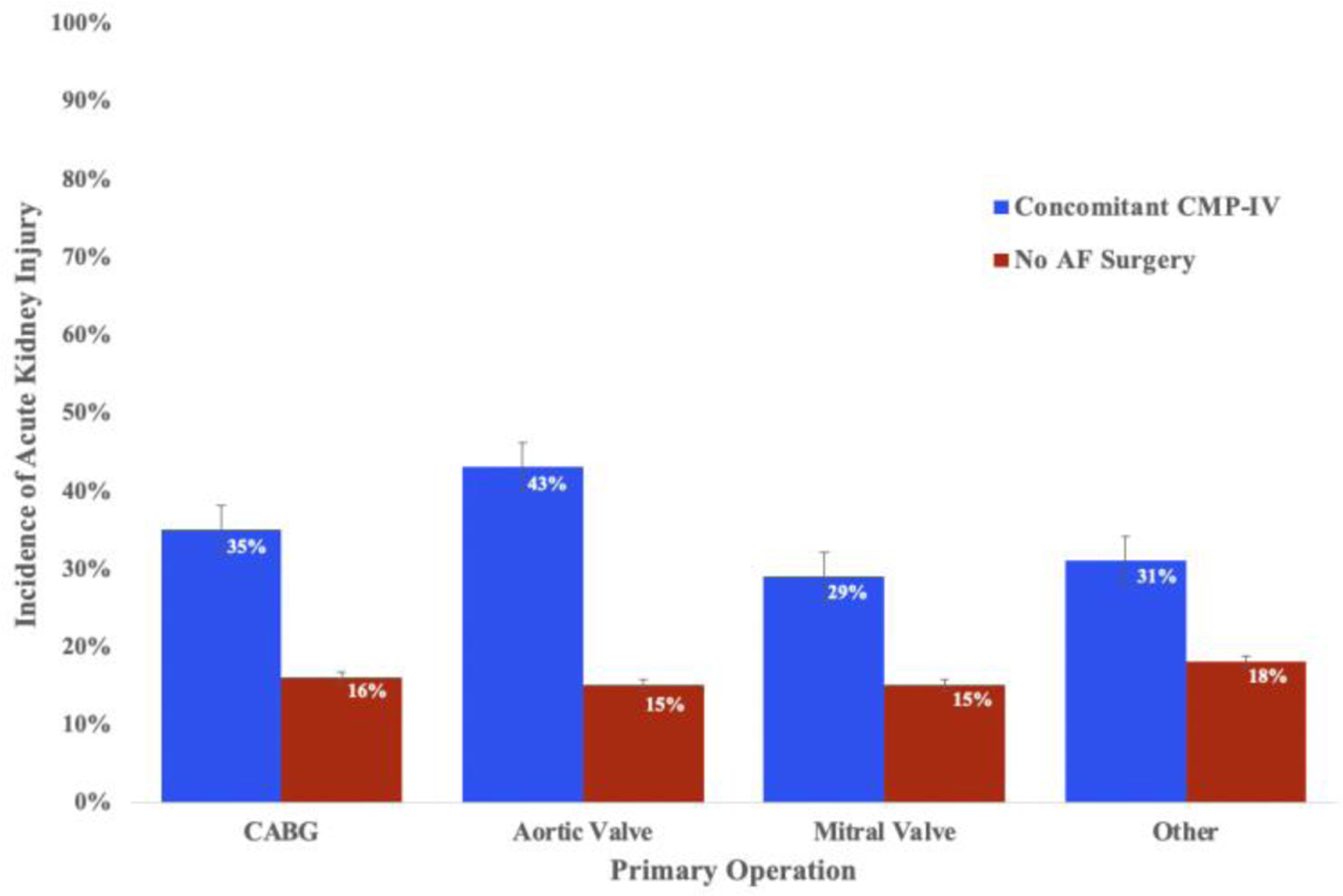
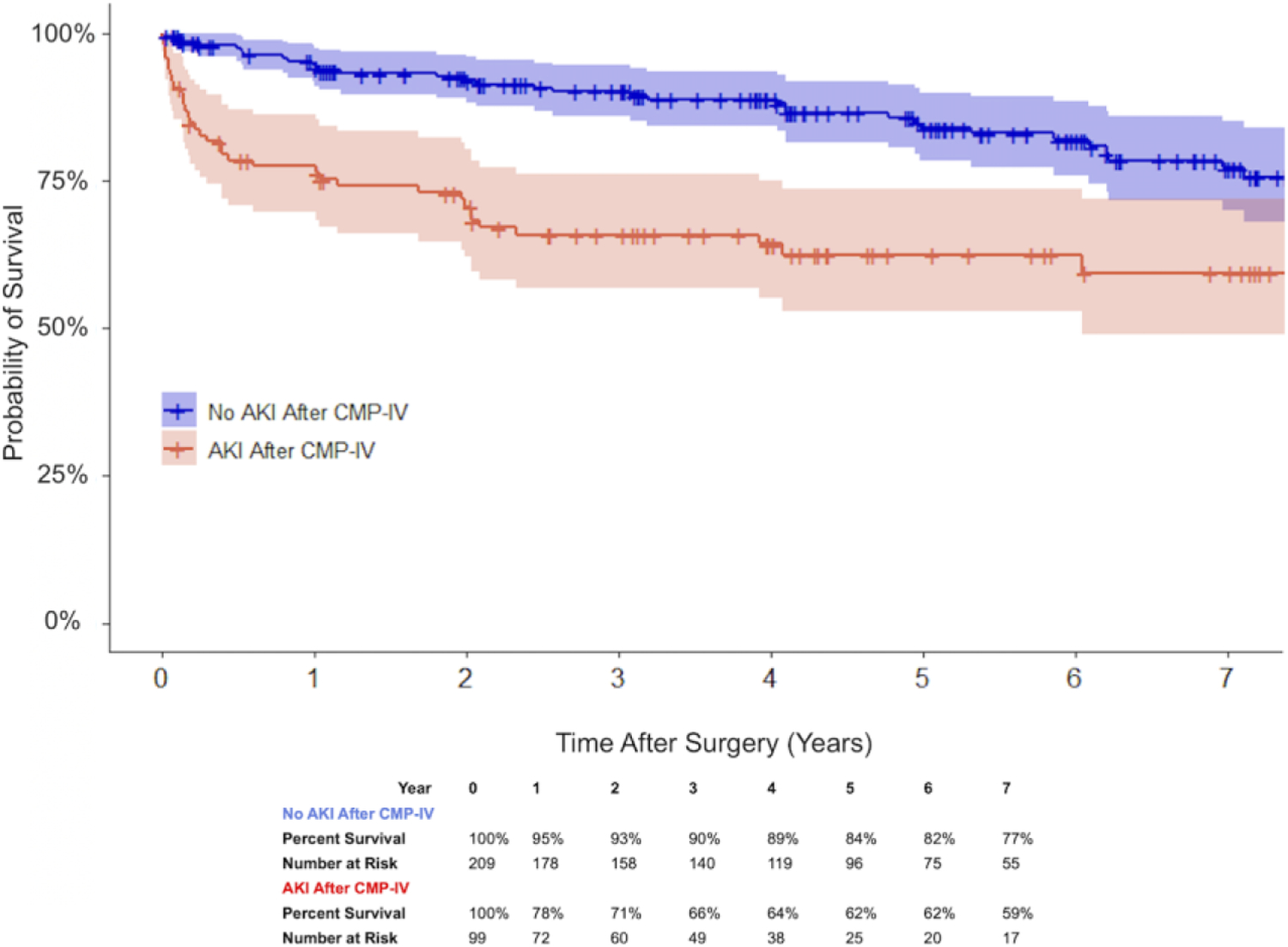
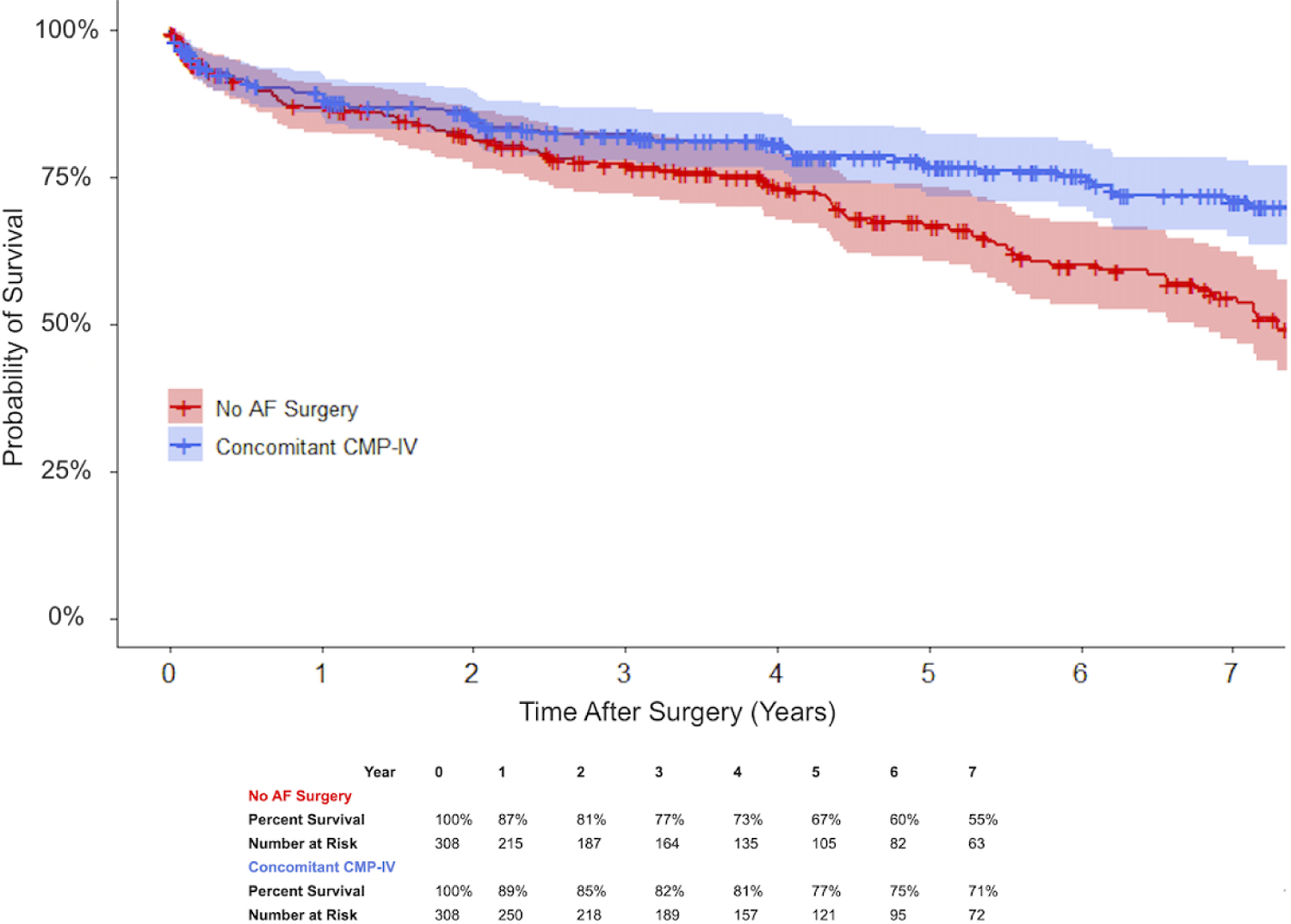
Results: Propensity matching yielded 308 patients in each group (n = 616). All preoperative variables were similar between groups. The concomitant CMP-IV group had a greater incidence of AKI: 32% (n = 99) versus 16% (n = 49), P < .001. After accounting for bypass time and nonablation operations on mixed effects analysis, concomitant CMP-IV was associated with increased risk of AKI (odds ratio, 1.89; confidence interval, 1.12-3.18; P = .017). While AKI was associated with decreased late survival (P < .001), patients who received a concomitant CMP-IV maintained superior 7-year survival to patients who received no ablation (P < .001). No patients required permanent dialysis.
Conclusions: Concomitant CMP-IV was independently associated with increased risk of AKI in the acute postoperative period. However, the long-term risks of AKI were offset by the significant survival benefit of CMP-IV. Concerns regarding new-onset renal dysfunction should not prohibit recommendation of this procedure in appropriate patients.
Keywords: Cox-Maze IV procedure; acute kidney injury; dialysis; propensity score match; renal failure; surgical ablation.
Copyright © 2021 The American Association for Thoracic Surgery. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of Interest Disclosure:
R.J.D. - AtriCure, Inc: Speaker and receives research funding; LivaNova, Inc.: Speaker. Medtronic: Consultant; Edwards Lifesciences: Speaker.
Figures
Comment in
-
Commentary: Concomitant atrial fibrillation ablation: The juice is worth the squeeze.J Thorac Cardiovasc Surg. 2022 Dec;164(6):1861-1862. doi: 10.1016/j.jtcvs.2021.01.077. Epub 2021 Jan 29. J Thorac Cardiovasc Surg. 2022. PMID: 33610362 No abstract available.
-
Commentary: Concomitant surgical ablation of atrial fibrillation significantly improves late survival.J Thorac Cardiovasc Surg. 2022 Dec;164(6):1859-1860. doi: 10.1016/j.jtcvs.2021.01.078. Epub 2021 Jan 29. J Thorac Cardiovasc Surg. 2022. PMID: 33622554 No abstract available.
-
Commentary: Are the atrial fibrillation ablation guidelines wrong?J Thorac Cardiovasc Surg. 2022 Dec;164(6):1858-1859. doi: 10.1016/j.jtcvs.2021.02.001. Epub 2021 Feb 5. J Thorac Cardiovasc Surg. 2022. PMID: 33678507 No abstract available.
References
-
- Rosner MH, Okusa MD. Acute kidney injury associated with cardiac surgery. Clin J Am Soc Nephrol 2006;1(1):19–32. - PubMed
-
- Lassnigg A, Schmidlin D, Mouhieddine M, et al. Minimal changes of serum creatinine predict prognosis in patients after cardiothoracic surgery: a prospective cohort study. J Am Soc Nephrol 2004;15(6):1597–605. - PubMed
-
- Laffey JG, Boylan JF, Cheng DCH. The systemic inflammatory response to cardiac surgery. Anesthesiol 2002;97:215–52. - PubMed
-
- Badhwar V, Rankin JS, Damiano RJ, et al. The Society of Thoracic Surgeons 2017 Clinical practice guidelines for the surgical treatment of atrial fibrillation. Ann Thorac Surg 2017;103(1):329–341. - PubMed
-
- Ad N, Damiano RJ, Badhwar V, et al. Expert consensus guidelines: Examining surgical ablation for atrial fibrillation. J Thorac Cardiovasc Surg 2017;153(6):1330–1354.e1. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
