

High flow oxygen and risk of mortality in patients with a suspected acute coronary syndrome: pragmatic, cluster randomised, crossover trial
- PMID: 33653685
- PMCID: PMC7923953
- DOI: 10.1136/bmj.n355
High flow oxygen and risk of mortality in patients with a suspected acute coronary syndrome: pragmatic, cluster randomised, crossover trial
Abstract
Objective: To determine the association between high flow supplementary oxygen and 30 day mortality in patients presenting with a suspected acute coronary syndrome (ACS).
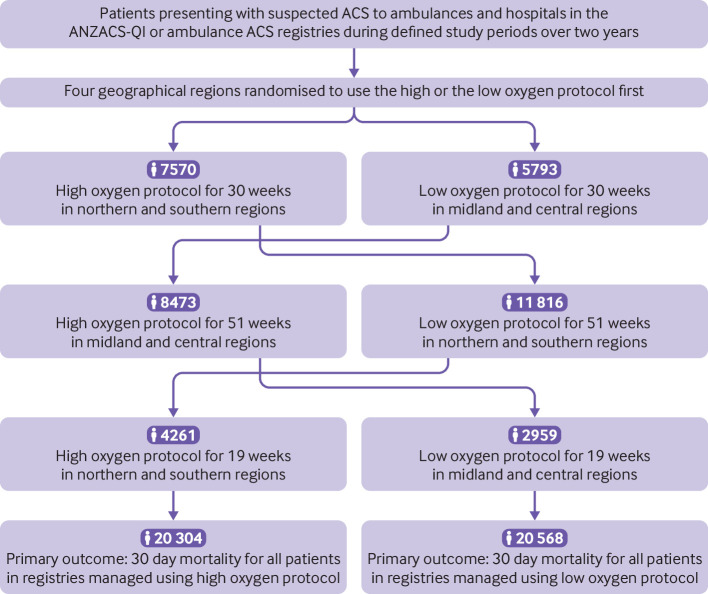
Design: Pragmatic, cluster randomised, crossover trial.
Setting: Four geographical regions in New Zealand.
Participants: 40 872 patients with suspected or confirmed ACS included in the All New Zealand Acute Coronary Syndrome Quality Improvement registry or ambulance ACS pathway during the study periods. 20 304 patients were managed using the high oxygen protocol and 20 568 were managed using the low oxygen protocol. Final diagnosis of ST elevation myocardial infarction (STEMI) and non-STEMI were determined from the registry and ICD-10 discharge codes.
Interventions: The four geographical regions were randomly allocated to each of two oxygen protocols in six month blocks over two years. The high oxygen protocol recommended oxygen at 6-8 L/min by face mask for ischaemic symptoms or electrocardiographic changes, irrespective of the transcapillary oxygen saturation (SpO2). The low oxygen protocol recommended oxygen only if SpO2 was less than 90%, with a target SpO2 of less than 95%.
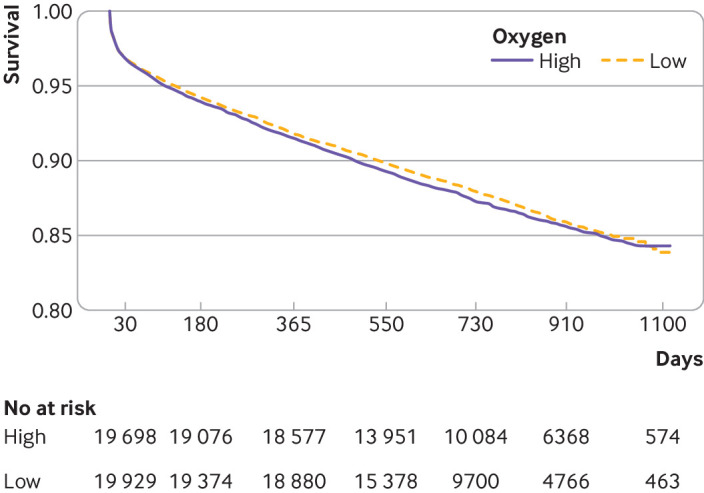
Main outcome measure: 30 day all cause mortality determined from linkage to administrative data.
Results: Personal and clinical characteristics of patients managed under both oxygen protocols were well matched. For patients with suspected ACS, 30 day mortality for the high and low oxygen groups was 613 (3.0%) and 642 (3.1%), respectively (odds ratio 0.97, 95% confidence interval 0.86 to 1.08). For 4159 (10%) patients with STEMI, 30 day mortality for the high and low oxygen groups was 8.8% (n=178) and 10.6% (n=225), respectively (0.81, 0.66 to 1.00) and for 10 218 (25%) patients with non-STEMI was 3.6% (n=187) and 3.5% (n=176), respectively (1.05, 0.85 to 1.29).
Conclusion: In a large patient cohort presenting with suspected ACS, high flow oxygen was not associated with an increase or decrease in 30 day mortality.
Trial registration: ANZ Clinical Trials ACTRN12616000461493.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: support from the National Heart Foundation of New Zealand (grant No 1649) and from the Health Research Council of New Zealand clinical practitioner fellowships to RAHS and MT; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years ; no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- Amsterdam EA, Wenger NK, Brindis RG, et al. ACC/AHA Task Force Members. Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons . 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. [correction in: Circulation 2014;130:e431-2.] Circulation 2014;130:2354-94. 10.1161/CIR.0000000000000133 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical