

Systematic review of prediction models for pulmonary tuberculosis treatment outcomes in adults
- PMID: 33653759
- PMCID: PMC7929865
- DOI: 10.1136/bmjopen-2020-044687
Systematic review of prediction models for pulmonary tuberculosis treatment outcomes in adults
Abstract
Objective: To systematically review and critically evaluate prediction models developed to predict tuberculosis (TB) treatment outcomes among adults with pulmonary TB.
Design: Systematic review.
Data sources: PubMed, Embase, Web of Science and Google Scholar were searched for studies published from 1 January 1995 to 9 January 2020.
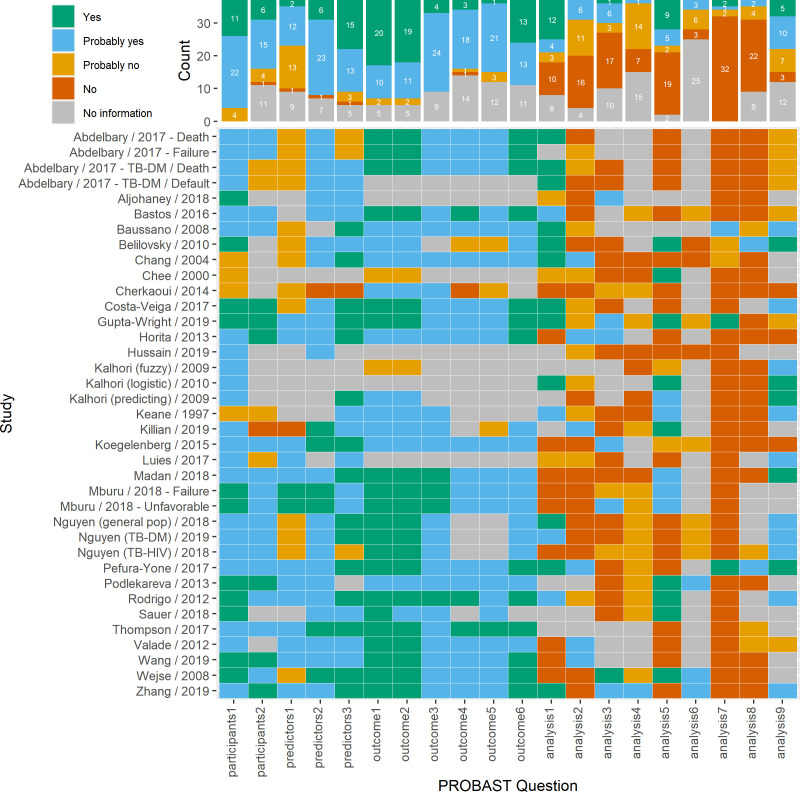
Study selection and data extraction: Studies that developed a model to predict pulmonary TB treatment outcomes were included. Study screening, data extraction and quality assessment were conducted independently by two reviewers. Study quality was evaluated using the Prediction model Risk Of Bias Assessment Tool. Data were synthesised with narrative review and in tables and figures.
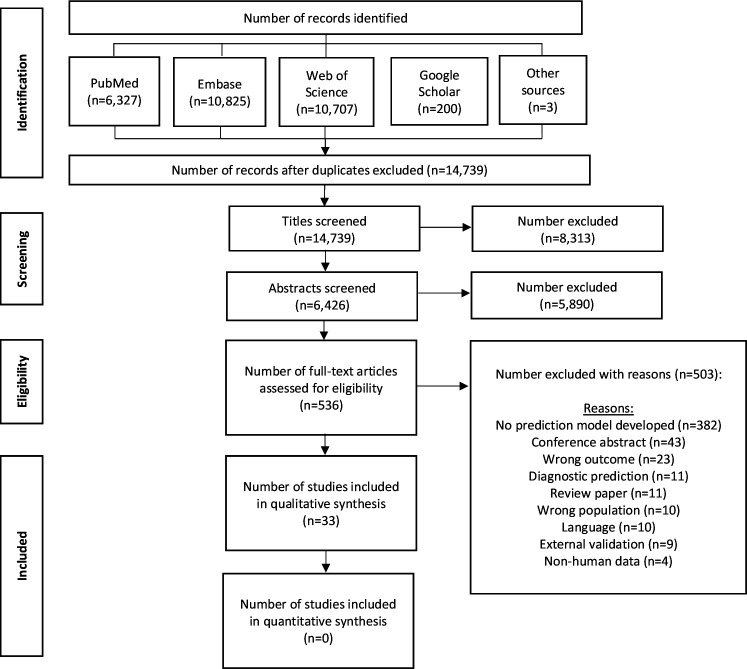
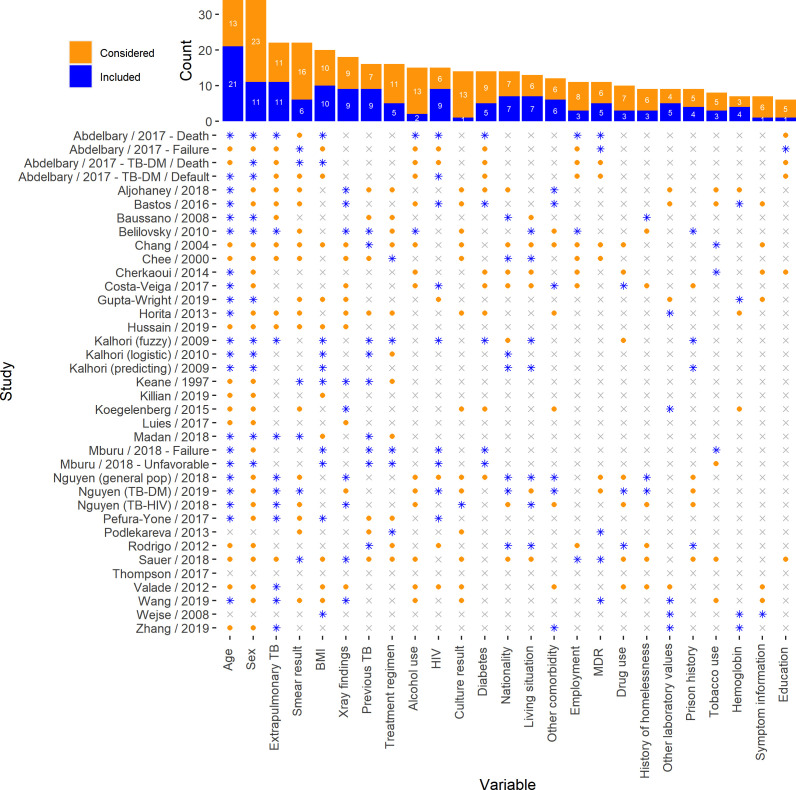
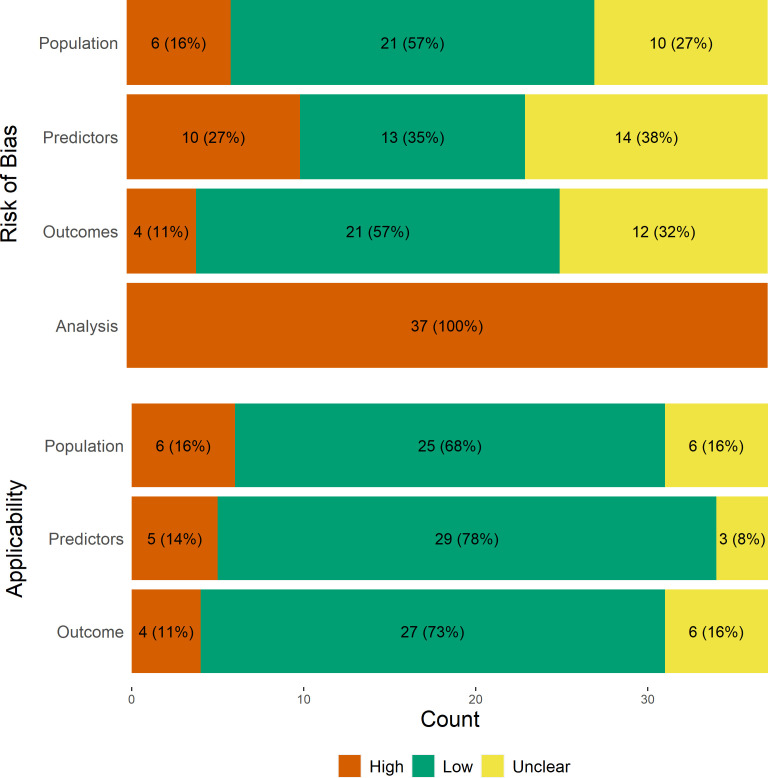
Results: 14 739 articles were identified, 536 underwent full-text review and 33 studies presenting 37 prediction models were included. Model outcomes included death (n=16, 43%), treatment failure (n=6, 16%), default (n=6, 16%) or a composite outcome (n=9, 25%). Most models (n=30, 81%) measured discrimination (median c-statistic=0.75; IQR: 0.68-0.84), and 17 (46%) reported calibration, often the Hosmer-Lemeshow test (n=13). Nineteen (51%) models were internally validated, and six (16%) were externally validated. Eighteen (54%) studies mentioned missing data, and of those, half (n=9) used complete case analysis. The most common predictors included age, sex, extrapulmonary TB, body mass index, chest X-ray results, previous TB and HIV. Risk of bias varied across studies, but all studies had high risk of bias in their analysis.
Conclusions: TB outcome prediction models are heterogeneous with disparate outcome definitions, predictors and methodology. We do not recommend applying any in clinical settings without external validation, and encourage future researchers adhere to guidelines for developing and reporting of prediction models.
Trial registration: The study was registered on the international prospective register of systematic reviews PROSPERO (CRD42020155782).
Keywords: epidemiology; statistics & research methods; tuberculosis.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- World Health Organization . Global tuberculosis report 2019. Geneva, 2019.
-
- World Health Organization . The end TB strategy. Geneva, 2015.
-
- Nahid P, Dorman SE, Alipanah N, et al. Official American thoracic Society/Centers for disease control and Prevention/Infectious diseases Society of America clinical practice guidelines: treatment of drug-susceptible tuberculosis. Clin Infect Dis 2016;63:e147–95. 10.1093/cid/ciw376 - DOI - PMC - PubMed
-
- World Health Organization . Guildelines for treatment of drug-susceptible tuberculosis and patient care. Licence: CC BY-NC-SA 3.0 IGO. Geneva: WHO/HTM/TB, 2017.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources