

Considerations for treatment duration in responders to immune checkpoint inhibitors
- PMID: 33653801
- PMCID: PMC7929825
- DOI: 10.1136/jitc-2020-001901
Considerations for treatment duration in responders to immune checkpoint inhibitors
Abstract
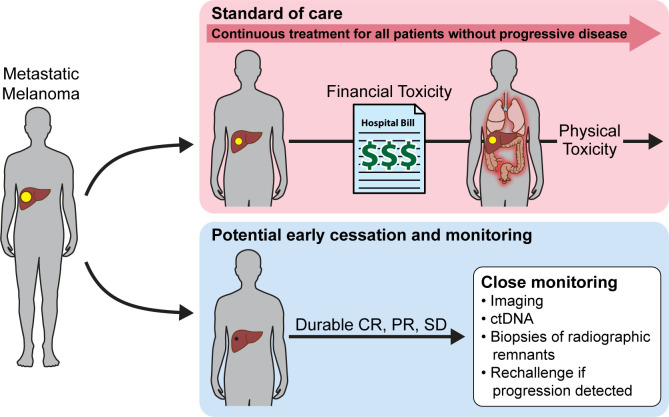
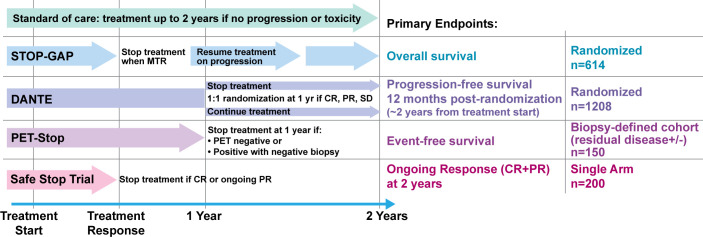
Immune checkpoint inhibitors (ICIs) have improved overall survival for cancer patients, however, optimal duration of ICI therapy has yet to be defined. Given ICIs were first used to treat patients with metastatic melanoma, a condition that at the time was incurable, little attention was initially paid to how much therapy would be needed for a durable response. As the early immunotherapy trials have matured past 10 years, a significant per cent of patients have demonstrated durable responses; it is now time to determine whether patients have been overtreated, and if durable remissions can still be achieved with less therapy, limiting the physical and financial toxicity associated with years of treatment. Well-designed trials are needed to identify optimal duration of therapy, and to define biomarkers to predict who would benefit from shorter courses of immunotherapy. Here, we outline key questions related to health, financial and societal toxicities of over treating with ICI and present four unique clinical trials aimed at exposing criteria for early cessation of ICI. Taken together, there is a serious liability to overtreating patients with ICI and future work is warranted to determine when it is safe to stop ICI.
Keywords: Costimulatory and Inhibitory T-Cell Receptors; Immunotherapy; Melanoma; Review.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: TM is a consultant for AstraZeneca, Genentech, Boehringe Ingelheim, Atara, and Regeneron. And receives research grant support from Bristol Myers Squibb, Regeneron, Merck, and Boehringer Ingelheim. AER receives sponsored research support from Janssen, AbbVie, Bristol Myers Squibb, Celgene SMR receives consulting fees from Eli Lilly, Daiichi Sankyo and Silverback Therapeutics and research support from Cancer Prevention and Research Institute of Texas RR190020. MER-R receives research grant support from ROCHE and Highlight Therapeutics. SC and CF are employees and shareholder at NanoString Technologies. DHA has received royalties from the University of Illinois and has received consulting fees from Boehringer Ingelheim. JG is a consultant for Glaxo-Smith Kline (GSK), Array BioPharma, Codagenix, Verseau Therapeutics and Kymera and receives sponsored research support from GSK, Eli Lilly and Array BioPharma.
Figures
References
-
- Pokorny R, McPherson JP, Grossmann KF, et al. . Clinical outcomes with early-elective discontinuation of PD-1 inhibitors (PDI) at one year in patients (PTS) with metastatic melanoma (Mm). Journal of Clinical Oncology 2020;38:10048. 10.1200/JCO.2020.38.15_suppl.10048 - DOI
-
- Schadendorf D, Wolchok JD, Hodi FS, et al. . Efficacy and safety outcomes in patients with advanced melanoma who discontinued treatment with nivolumab and ipilimumab because of adverse events: a pooled analysis of randomized phase II and III trials. J Clin Oncol 2017;35:3807–14. 10.1200/JCO.2017.73.2289 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous