

The pathogenesis and diagnosis of sepsis post burn injury
- PMID: 33654698
- PMCID: PMC7901709
- DOI: 10.1093/burnst/tkaa047
The pathogenesis and diagnosis of sepsis post burn injury
Abstract
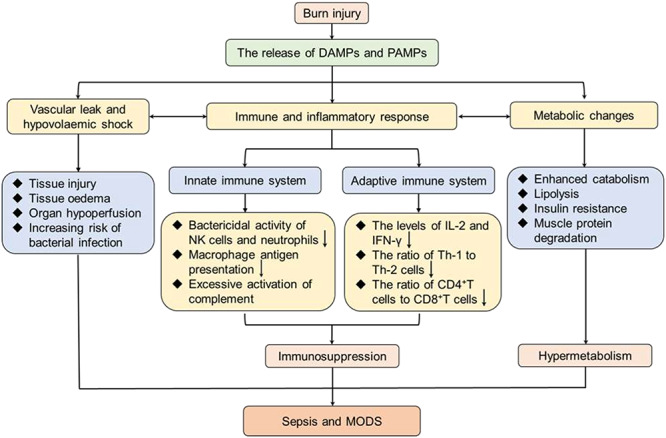
Burn is an under-appreciated trauma that is associated with unacceptably high morbidity and mortality. Although the survival rate after devastating burn injuries has continued to increase in previous decades due to medical advances in burn wound care, nutritional and fluid resuscitation and improved infection control practices, there are still large numbers of patients at a high risk of death. One of the most common complications of burn is sepsis, which is defined as "severe organ dysfunction attributed to host's disordered response to infection" and is the primary cause of death in burn patients. Indeed, burn injuries are accompanied by a series of events that lead to sepsis and multiple organ dysfunction syndrome, such as a hypovolaemic state, immune and inflammatory responses and metabolic changes. Therefore, clear diagnostic criteria and predictive biomarkers are especially important in the prevention and treatment of sepsis and septic shock. In this review, we focus on the pathogenesis of burn wound infection and the post-burn events leading to sepsis. Moreover, the clinical and promising biomarkers of burn sepsis will also be summarized.
Keywords: Biomaker; Burn; Hypermetabolism; Immune dysregulation; Infection; Inflammation; Multiple organ dysfunction syndrome; Sepsis; Septic shock; Trauma.
© The Author(s) 2021. Published by Oxford University Press.
Figures

References
-
- National Burn Repository 2019 Update , Report of data from 2009–2018 ameriburn.site- ym.com [Internet]. 2019. Available from: https://ameriburn.site-ym.com/store/ViewProduct.aspx?id=14191872.
-
- Pereira RF, Barrias CC, Granja PL, Bartolo PJ. Advanced biofabrication strategies for skin regeneration and repair. Nanomedicine (Lond.) 2013;8:603–21. - PubMed
-
- Peck MD. Epidemiology of burns throughout the world. Part I: distribution and risk factors. Burns 2011;37:1087–100. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
