

Estimating risk of mechanical ventilation and in-hospital mortality among adult COVID-19 patients admitted to Mass General Brigham: The VICE and DICE scores
- PMID: 33655204
- PMCID: PMC7906522
- DOI: 10.1016/j.eclinm.2021.100765
Estimating risk of mechanical ventilation and in-hospital mortality among adult COVID-19 patients admitted to Mass General Brigham: The VICE and DICE scores
Abstract
Background: Risk stratification of COVID-19 patients upon hospital admission is key for their successful treatment and efficient utilization of hospital resources. We sought to evaluate the risk factors on admission (including comorbidities, vital signs, and initial laboratory assessment) associated with ventilation need and in-hospital mortality in COVID-19.
Methods: We established a retrospective cohort of COVID-19 patients from Mass General Brigham hospitals. Demographic, clinical, and admission laboratory data were obtained from electronic medical records of patients admitted to the hospital with laboratory-confirmed COVID-19 before May 19, 2020. Multivariable logistic regression analyses were used to construct and validate the Ventilation in COVID Estimator (VICE) and Death in COVID Estimator (DICE) risk scores.
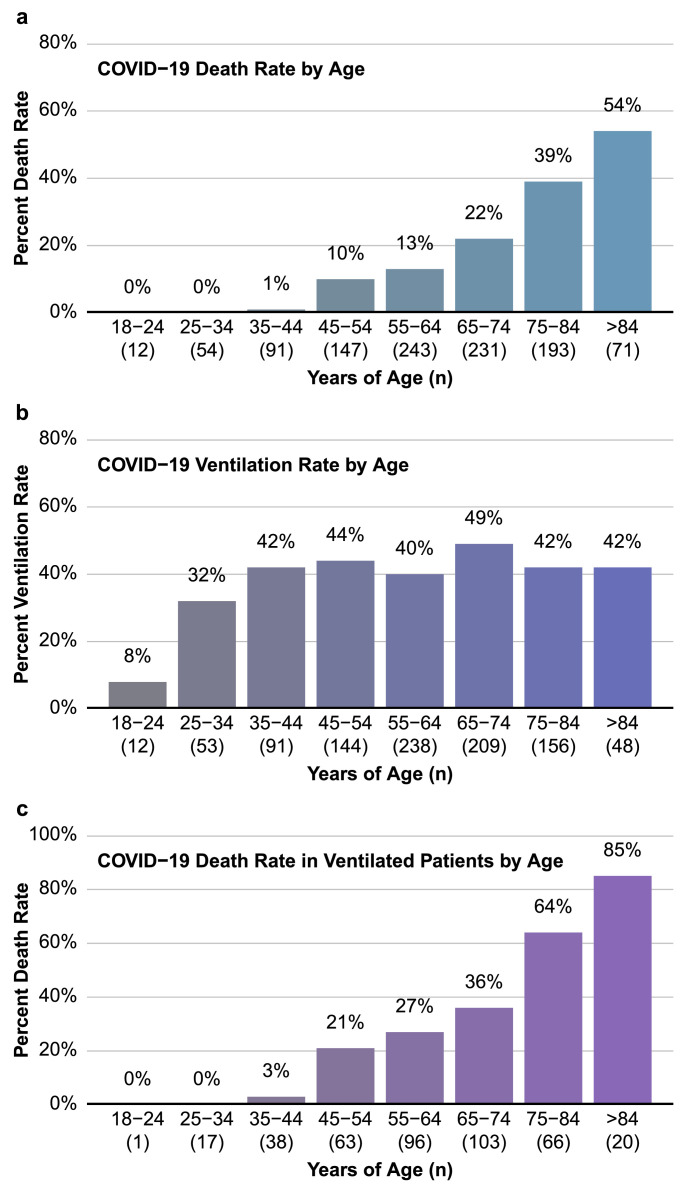
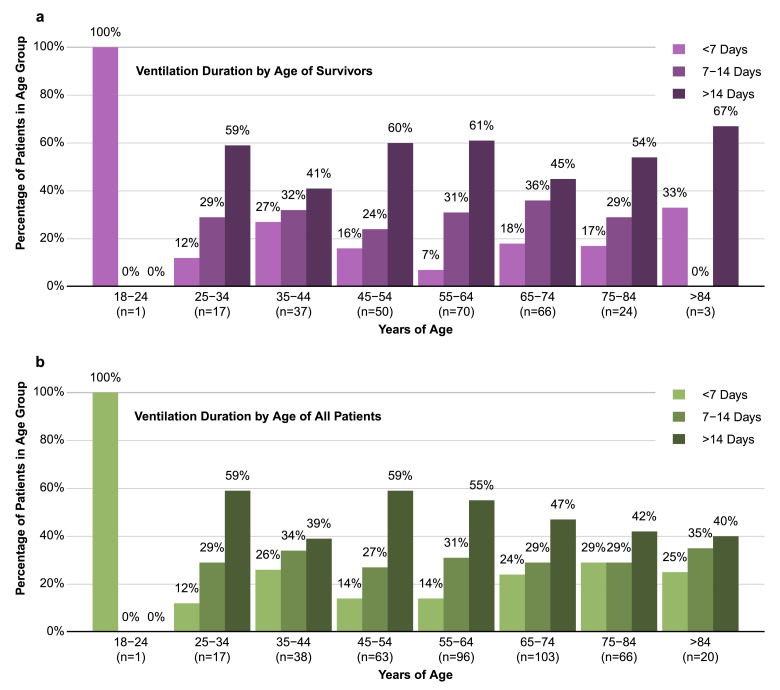
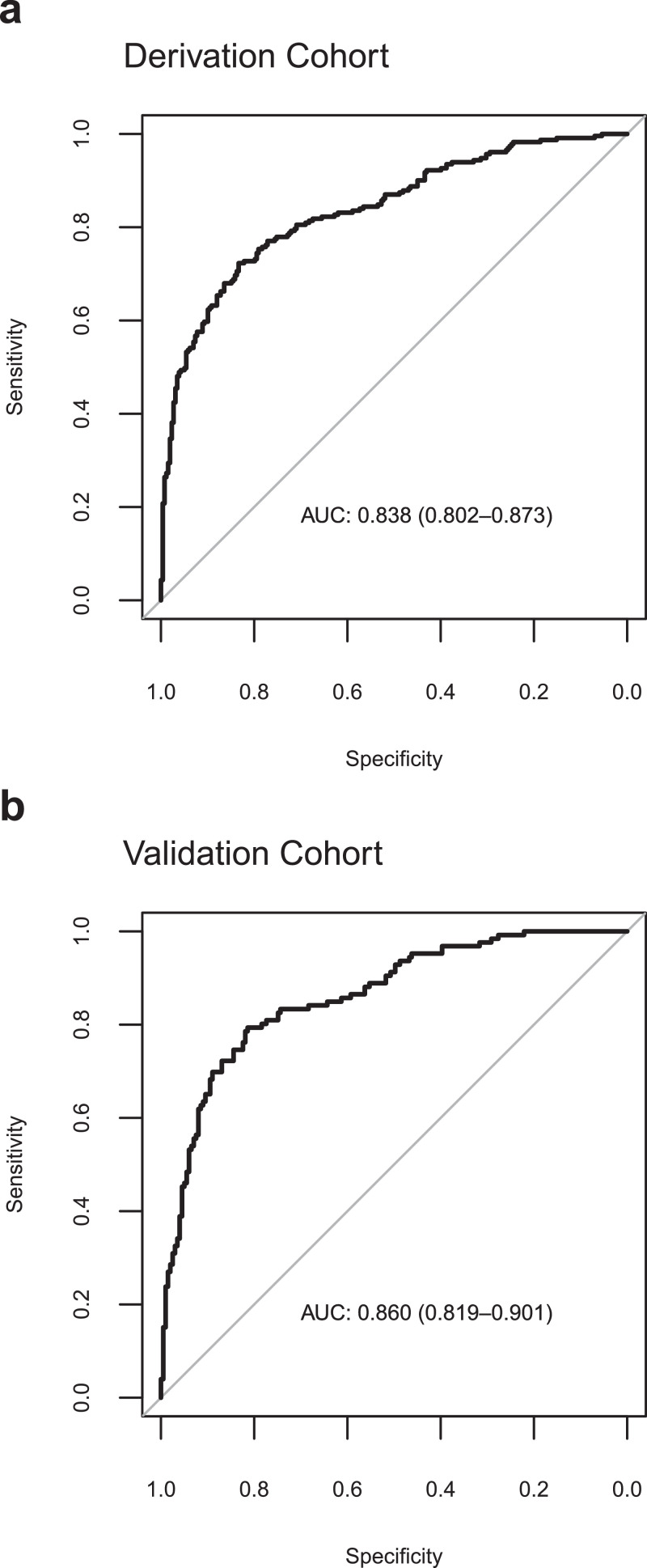
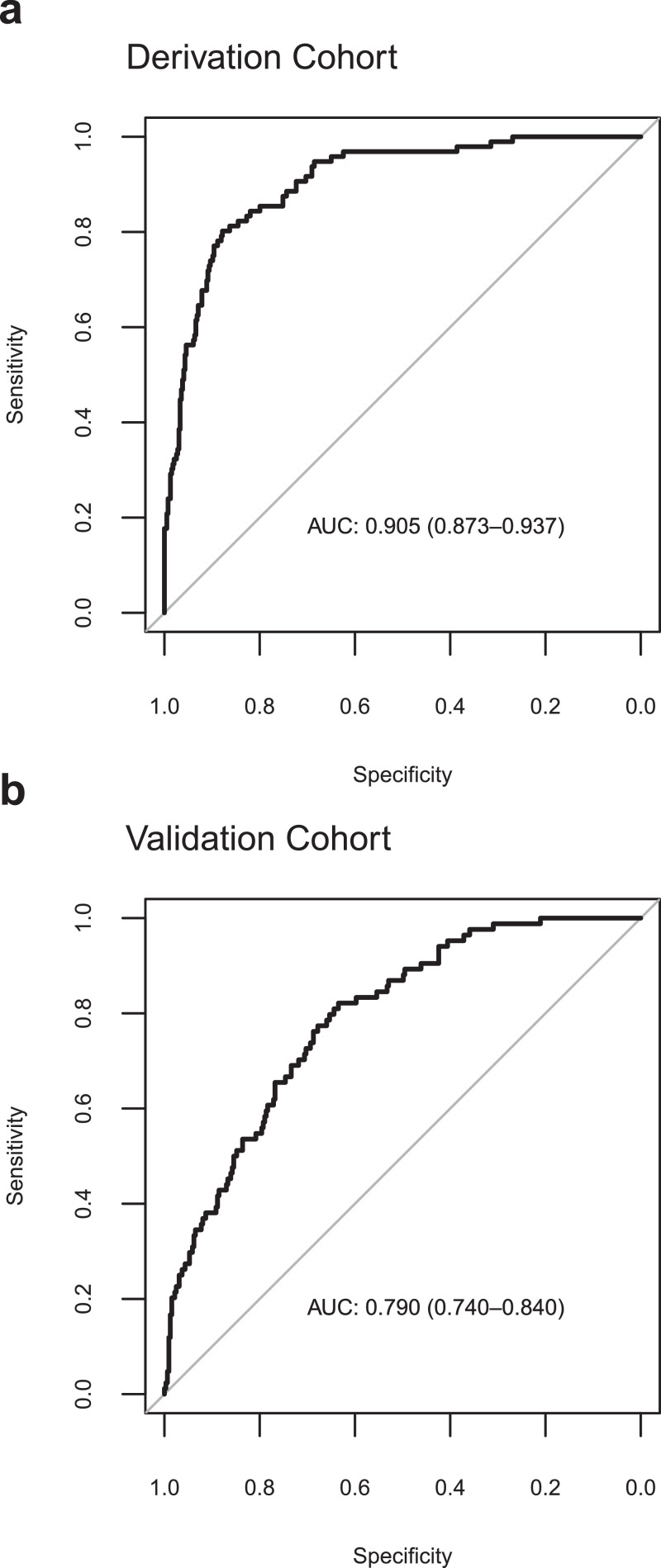
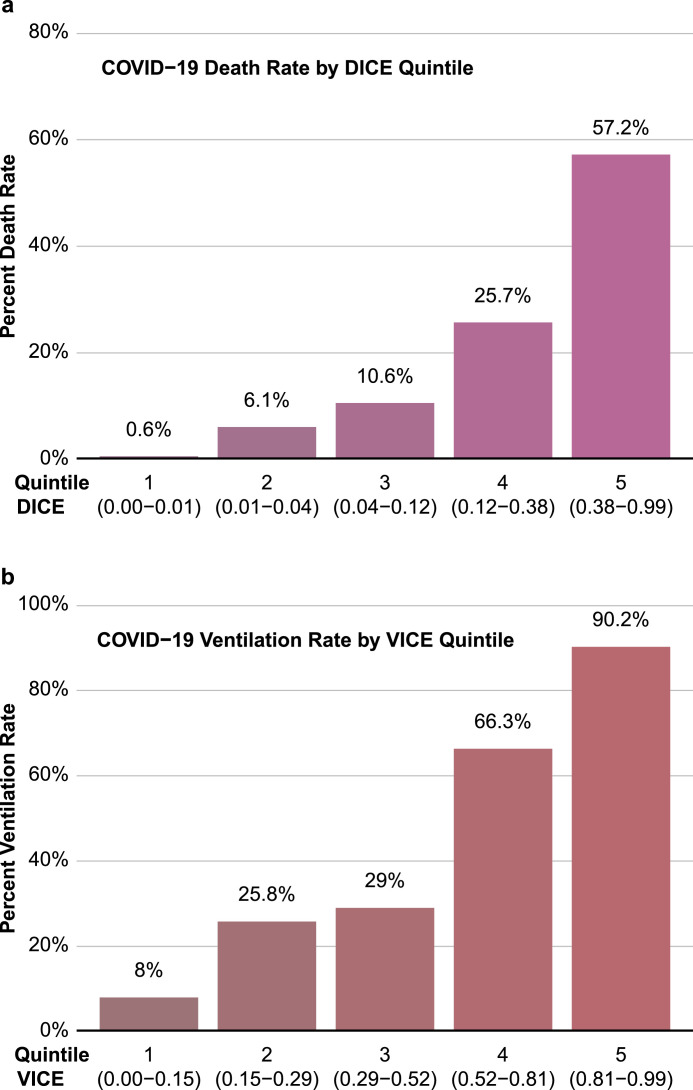
Findings: The entire cohort included 1042 patients (median age, 64 years; 56.8% male). The derivation and validation cohorts for the risk scores included 578 and 464 patients, respectively. We found four factors to be independently predictive for mechanical ventilation requirement (diabetes mellitus, SpO2:FiO2 ratio, C-reactive protein, and lactate dehydrogenase), and 10 factors to be predictors of in-hospital mortality (age, male sex, coronary artery disease, diabetes mellitus, chronic statin use, SpO2:FiO2 ratio, body mass index, neutrophil to lymphocyte ratio, platelet count, and procalcitonin). Using these factors, we constructed the VICE and DICE risk scores, which performed with C-statistics of 0.84 and 0.91, respectively. Importantly, the chronic use of a statin was associated with protection against death due to COVID-19. The VICE and DICE score calculators have been placed on an interactive website freely available to healthcare providers and researchers (https://covid-calculator.com/).
Interpretation: The risk scores developed in this study may help clinicians more appropriately determine which COVID-19 patients will need to be managed with greater intensity.
Funding: COVID-19 Fast Grant (fastgrants.org).
© 2021 The Author(s).
Conflict of interest statement
All authors have nothing to disclose.
Figures
Update of
-
Estimating Risk of Mechanical Ventilation and Mortality Among Adult COVID-19 patients Admitted to Mass General Brigham: The VICE and DICE Scores.medRxiv [Preprint]. 2020 Sep 16:2020.09.14.20194670. doi: 10.1101/2020.09.14.20194670. medRxiv. 2020. Update in: EClinicalMedicine. 2021 Mar;33:100765. doi: 10.1016/j.eclinm.2021.100765. PMID: 32995802 Free PMC article. Updated. Preprint.
References
-
- University J.H. Coronavirus resource center. https://coronavirus.jhu.edu/. Published 2020. Accessed 12/15/2020, 2020.
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
