

This is a preprint.
Self-contained system for mitigation of contaminated aerosol sources of SARS-CoV-2
- PMID: 33655242
- PMCID: PMC7924284
- DOI: 10.21203/rs.3.rs-237873/v1
Self-contained system for mitigation of contaminated aerosol sources of SARS-CoV-2
Abstract
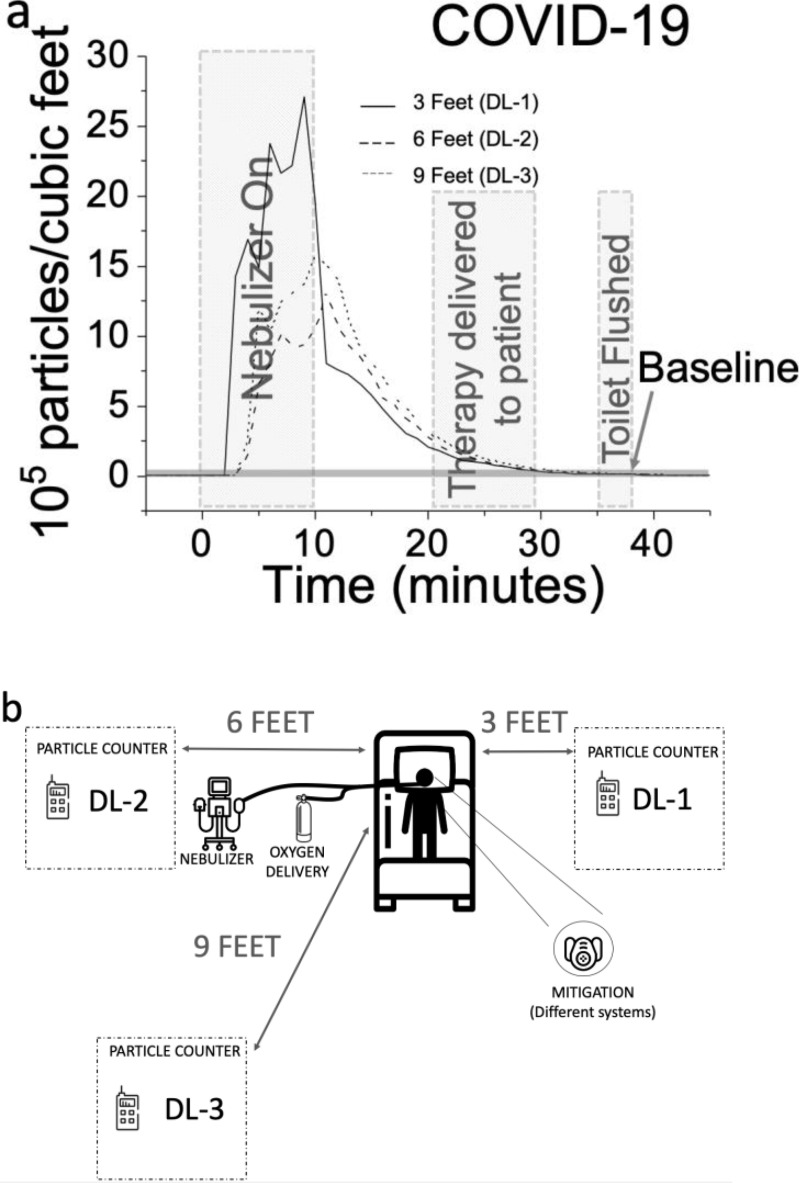
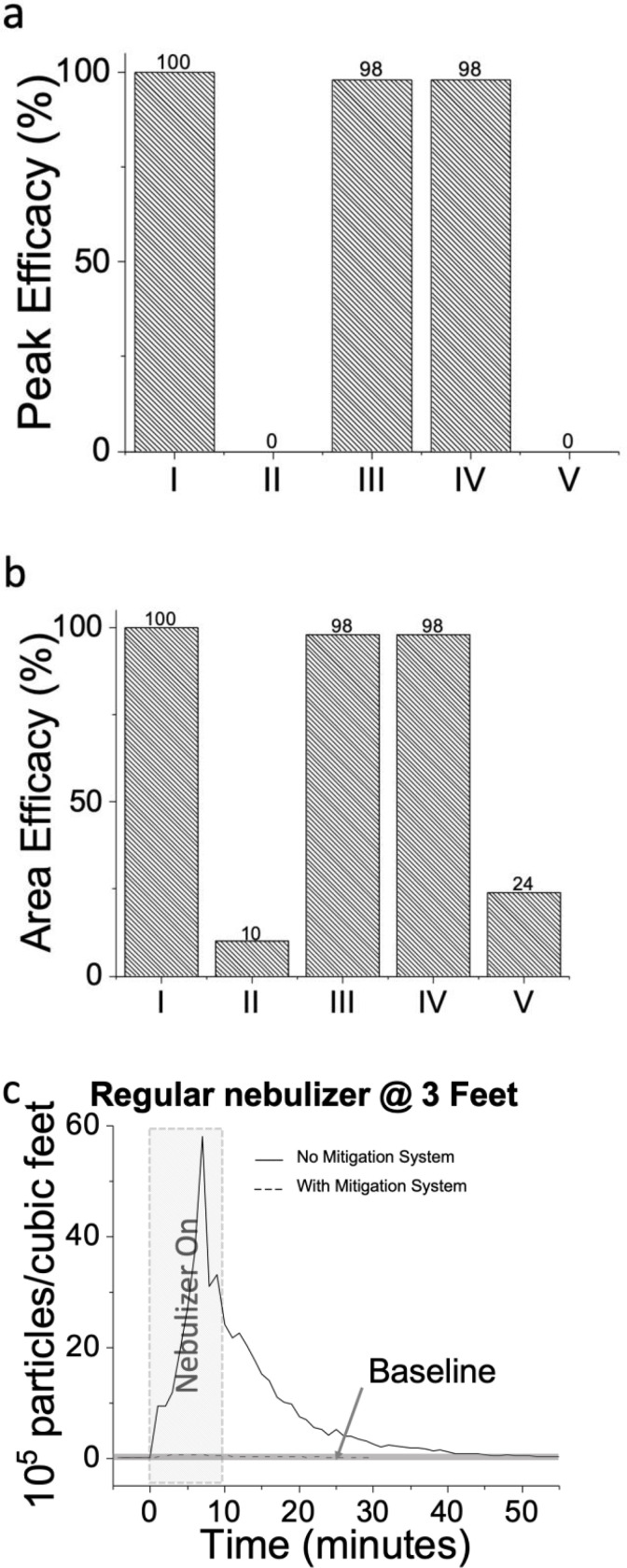
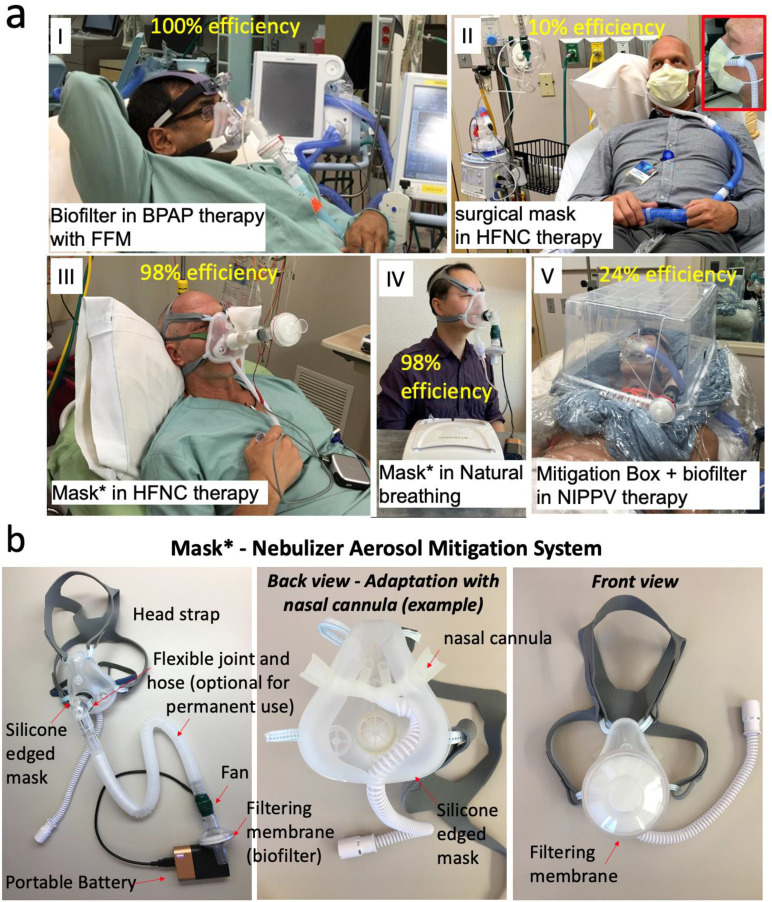
Contaminated aerosols and micro droplets are easily generated by infected hosts through sneezing, coughing, speaking and breathing1-3 and harm humans' health and the global economy. While most of the efforts are usually targeted towards protecting individuals from getting infected,4 eliminating transmissions from infection sources is also important to prevent disease transmission. Supportive therapies for Severe Acute Respiratory Syndrome Coronavirus 2 (SARS CoV-2) pneumonia such as oxygen supplementation, nebulizers and non-invasive mechanical ventilation all carry an increased risk for viral transmission via aerosol to healthcare workers.5-9 In this work, we study the efficacy of five methods for self-containing aerosols emitted from infected subjects undergoing nebulization therapies with a diverse spectrum on oxygen delivery therapies. The work includes five study cases: Case I: Use of a Full-Face Mask with biofilter in bilevel positive airway pressure device (BPAP) therapy, Case II: Use of surgical mask in High Flow Nasal Cannula (HFNC) therapy, Case III: Use of a modified silicone disposable mask in a HFNC therapy, Case IV: Use of a modified silicone disposable mask with a regular nebulizer and normal breathing, Case V: Use of a mitigation box with biofilter in a Non-Invasive Positive Pressure Ventilator (NIPPV). We demonstrate that while cases I, III and IV showed efficacies of 98-100%; cases II and V, which are the most commonly used, resulted with significantly lower efficacies of 10-24% to mitigate the dispersion of nebulization aerosols. Therefore, implementing cases I, III and IV in health care facilities may help battle the contaminations and infections via aerosol transmission during a pandemic.
Conflict of interest statement
Conflict of Interest: All authors, except XX and EF declare no conflict of interest. XX and EF are associated with TF Health Co. (d.b.a. Breezing Co.).
Figures
Similar articles
-
Mitigating Fugitive Aerosols During Aerosol Delivery via High-Flow Nasal Cannula Devices.Respir Care. 2022 Apr;67(4):404-414. doi: 10.4187/respcare.09589. Epub 2021 Nov 17. Respir Care. 2022. PMID: 34789564
-
[Standard technical specifications for methacholine chloride (Methacholine) bronchial challenge test (2023)].Zhonghua Jie He He Hu Xi Za Zhi. 2024 Feb 12;47(2):101-119. doi: 10.3760/cma.j.cn112147-20231019-00247. Zhonghua Jie He He Hu Xi Za Zhi. 2024. PMID: 38309959 Chinese.
-
Aerosol Generation from the Respiratory Tract with Various Modes of Oxygen Delivery.Am J Respir Crit Care Med. 2020 Oct 15;202(8):1115-1124. doi: 10.1164/rccm.202006-2309OC. Am J Respir Crit Care Med. 2020. PMID: 32822208 Free PMC article.
-
Airborne transmission of severe acute respiratory syndrome coronavirus-2 to healthcare workers: a narrative review.Anaesthesia. 2020 Aug;75(8):1086-1095. doi: 10.1111/anae.15093. Epub 2020 May 8. Anaesthesia. 2020. PMID: 32311771 Free PMC article. Review.
-
High-flow nasal cannula for acute hypoxemic respiratory failure in patients with COVID-19: systematic reviews of effectiveness and its risks of aerosolization, dispersion, and infection transmission.Can J Anaesth. 2020 Sep;67(9):1217-1248. doi: 10.1007/s12630-020-01740-2. Epub 2020 Jun 15. Can J Anaesth. 2020. PMID: 32542464 Free PMC article.
References
-
- Santarpia J.L. et al. Aerosol and Surface Transmission Potential of SARS-CoV-2. medRxiv 2020.03.23., 10.1101/2020.1103.1123.20039446 (2020). - DOI
-
- Li Y. et al. Role of ventilation in airborne transmission of infectious agents in the built environment – a multidisciplinary systematic review. Indoor Air, Internationa Journal of Indoor Environment and Health 17, 2–18 (2007). - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
