

This is a preprint.
The SARS-CoV-2 antibody landscape is lower in magnitude for structural proteins, diversified for accessory proteins and stable long-term in children
- PMID: 33655259
- PMCID: PMC7924280
- DOI: 10.1101/2021.01.03.21249180
The SARS-CoV-2 antibody landscape is lower in magnitude for structural proteins, diversified for accessory proteins and stable long-term in children
Abstract
Background: Children are less clinically affected by SARS-CoV-2 infection than adults with the majority of cases being mild or asymptomatic and the differences in infection outcomes are poorly understood. The kinetics, magnitude and landscape of the antibody response may impact the clinical severity and serological diagnosis of COVID-19. Thus, a comprehensive investigation of the antibody landscape in children and adults is needed.
Methods: We tested 254 plasma from 122 children with symptomatic and asymptomatic SARS-CoV-2 infections in Hong Kong up to 206 days post symptom onset, including 146 longitudinal samples from 58 children. Adult COVID-19 patients and pre-pandemic controls were included for comparison. We assessed antibodies to a 14-wide panel of SARS-CoV-2 structural and accessory proteins by Luciferase Immunoprecipitation System (LIPS).
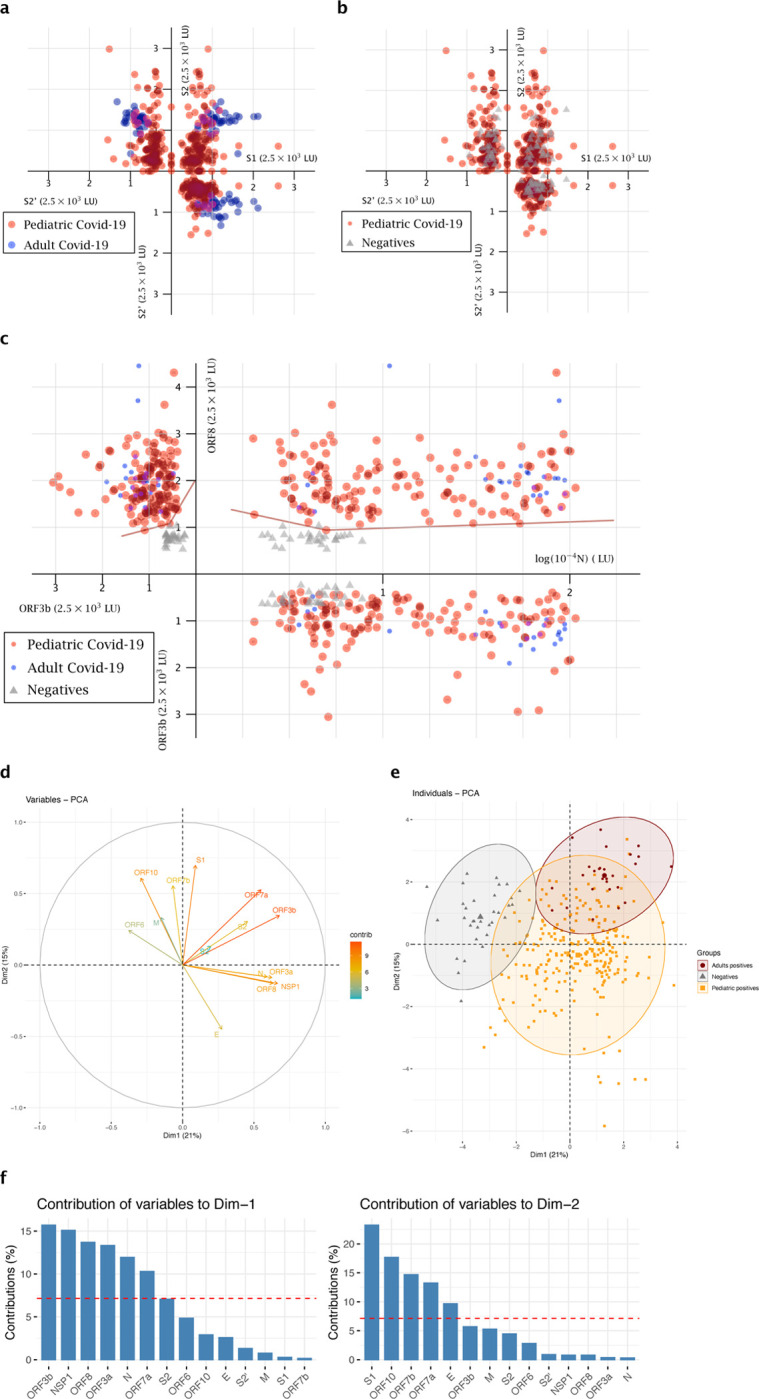
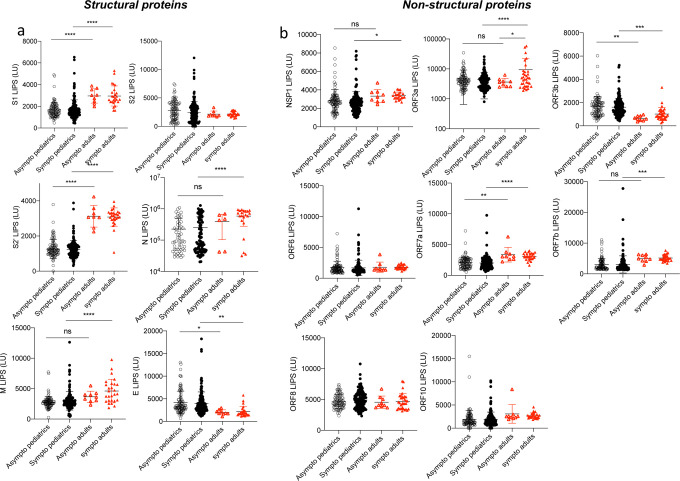
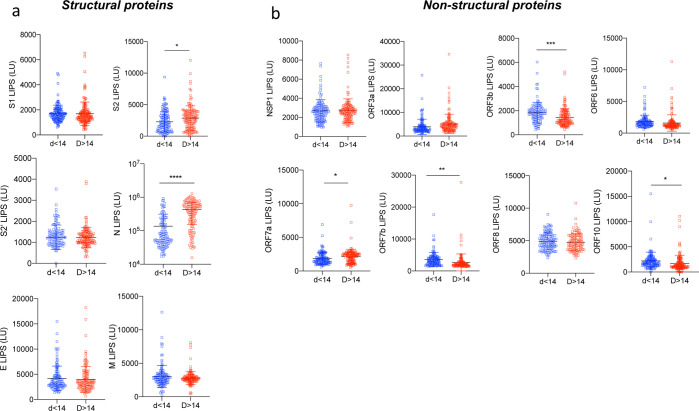
Findings: Children have lower levels of Spike and Nucleocapsid antibodies than adults, and their cumulative humoral response is more expanded to accessory proteins (NSP1 and Open Reading Frames (ORFs)). Sensitive serology using the three N, ORF3b, ORF8 antibodies can discriminate COVID-19 in children. Principal component analysis revealed distinct serological signatures in children and the highest contribution to variance were responses to non-structural proteins ORF3b, NSP1, ORF7a and ORF8. Longitudinal sampling revealed maintenance or increase of antibodies for at least 6 months, except for ORF7b antibodies which showed decline. It was interesting to note that children have higher antibody responses towards known IFN antagonists: ORF3b, ORF6 and ORF7a. The diversified SARS-CoV-2 antibody response in children may be an important factor in driving control of SARS-CoV-2 infection.
Keywords: Antibody; COVID-19; IFN; accessory; asymptomatic; longitudinal; pediatric; structural.
Conflict of interest statement
Competing interests A Hachim, N Kavian, LLM Poon, JSM Peiris and SA Valkenburg have filed an IDF (US 63/016,898) for the use of ORF8 and ORF3b as diagnostics of SARS-CoV-2 infection.
Figures




Similar articles
-
SARS-CoV-2 accessory proteins reveal distinct serological signatures in children.Nat Commun. 2022 May 26;13(1):2951. doi: 10.1038/s41467-022-30699-5. Nat Commun. 2022. PMID: 35618731 Free PMC article.
-
The role of SARS-CoV-2 accessory proteins in immune evasion.Biomed Pharmacother. 2022 Dec;156:113889. doi: 10.1016/j.biopha.2022.113889. Epub 2022 Oct 17. Biomed Pharmacother. 2022. PMID: 36265309 Free PMC article. Review.
-
ORF8 and ORF3b antibodies are accurate serological markers of early and late SARS-CoV-2 infection.Nat Immunol. 2020 Oct;21(10):1293-1301. doi: 10.1038/s41590-020-0773-7. Epub 2020 Aug 17. Nat Immunol. 2020. PMID: 32807944
-
Target genes used for biosensor development in COVID-19 diagnosis.Biosens Bioelectron. 2022 Mar 15;200:113924. doi: 10.1016/j.bios.2021.113924. Epub 2021 Dec 30. Biosens Bioelectron. 2022. PMID: 34974265 Free PMC article. Review.
-
SARS-CoV-2 Proteins: Are They Useful as Targets for COVID-19 Drugs and Vaccines?Curr Mol Med. 2022;22(1):50-66. doi: 10.2174/1566524021666210223143243. Curr Mol Med. 2022. PMID: 33622224 Review.
Cited by
-
A cross-sectional investigation of SARS-CoV-2 seroprevalence and associated risk factors in children and adolescents in the United States.PLoS One. 2021 Nov 8;16(11):e0259823. doi: 10.1371/journal.pone.0259823. eCollection 2021. PLoS One. 2021. PMID: 34748615 Free PMC article.
References
-
- Jones T.C., M. B., Veith T., Biele Guido, Zuchowski Marta, Hoffmann Jörg, Stein Angela, Edelmann Anke, Corman Victor Max, Drosten Christian. An analysis of SARS-CoV-2 viral load by patient age. medRxiv (2020).
-
- Valverde I., et al. Acute Cardiovascular Manifestations in 286 Children with Multisystem Inflammatory Syndrome Associated with COVID-19 Infection in Europe. Circulation (2020). - PubMed
-
- Zimmermann P. & Curtis N. Why is COVID-19 less severe in children? A review of the proposed mechanisms underlying the age-related difference in severity of SARS-CoV-2 infections. Arch Dis Child (2020). - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous