

Regularity and Continuity of GP Contacts and Use of Statins Amongst People at Risk of Cardiovascular Events
- PMID: 33655384
- PMCID: PMC8175539
- DOI: 10.1007/s11606-021-06638-3
Regularity and Continuity of GP Contacts and Use of Statins Amongst People at Risk of Cardiovascular Events
Abstract
Background: Regularity and continuity of general practitioner (GP) contacts are associated with reduced hospitalisation. Opportunities for improved medication management are cited as a potential cause.
Objective: Determine associations between continuity and regularity of primary care and statin use amongst individuals at risk of cardiovascular disease (CVD) outcomes.
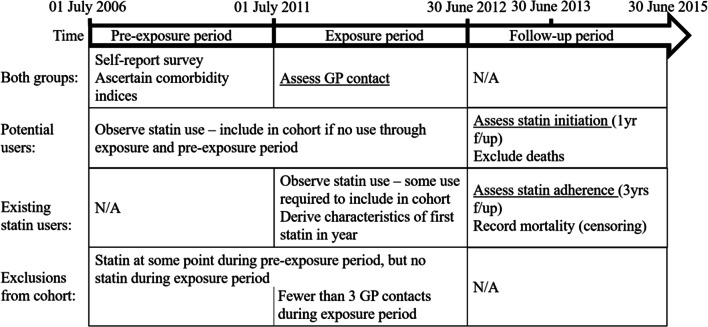
Design: Observational cohort study using self-report and administrative data from 267,153 participants of the Sax Institute's 45 and Up Study conducted in New South Wales, Australia. from 2006 to 2009. Medicare Benefits Schedule (MBS) and Pharmaceutical Benefits Scheme (PBS) data, from Services Australia, were linked to survey, hospital and death data by the NSW Centre for Health Record Linkage.
Participants: The 45 and Up Study participants at risk of CVD outcomes based on self-report and administrative data, divided into existing users and potential users based on dispensing records through the exposure period.
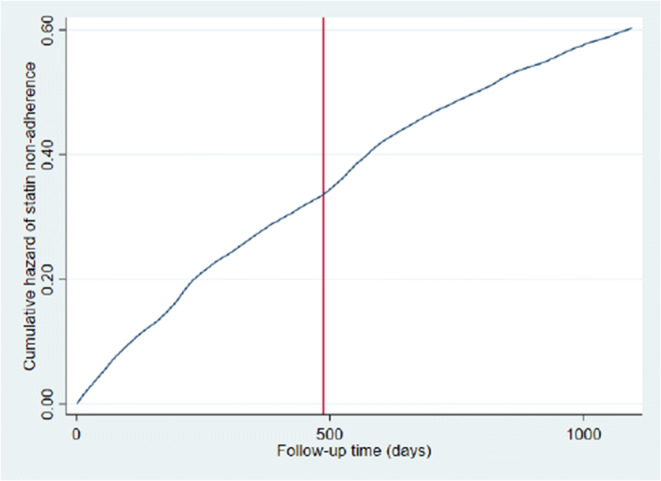
Main measures: The Continuity of Care index (COC), measuring whether patients see the same GP, and an index assessing whether GP visits are on a regular basis, measured from July 2011 to June 2012. Amongst potential users, statin initiation from July 2012 to June 2013 was assessed using logistic regression; amongst existing users, adherence was assessed from July 2012 to June 2015 using Cox regression (non-adherence being 30 days without statins).
Key results: Amongst 29,420 potential users, the most regular quintile had 1.22 times the odds of initiating statin (95%CI 1.11-1.34), while the high continuity group had an odds ratio of 1.12 (95%CI 1.02-1.24). Amongst 30,408 existing users, the most regular quintile had 0.82 the hazard of non-adherence (95%CI 0.78-0.87); the high continuity group had a hazard ratio of 0.89 (95%CI 0.84-0.94).
Conclusions: Regularity and continuity of care impact on medication management. It is possible that this mediates impacts on hospitalisation. Where there is a risk of unobserved confounding, potential causal pathways should be investigated.
Keywords: adherence; continuity of care; general practice; statins.
Conflict of interest statement
The authors declare that they do not have a conflict of interest.
Figures
References
-
- Hennen BK. Continuity of Care in Family Practice, Part 1: Dimensions of Continuity. Journal of Family Practice. 1975;2(5):371–2. - PubMed
-
- Hong JS, Kang HC. Continuity of ambulatory care and health outcomes in adult patients with type 2 diabetes in Korea. Health Policy. 2013;109(2):158–65. - PubMed
-
- Romaire MA, Haber SG, Wensky SG, McCall N. Primary care and specialty providers: an assessment of continuity of care, utilization, and expenditures. Medical Care. 2014;52(12):1042–9. - PubMed
-
- Barker I, Steventon A, Deeny SR. Association between continuity of care in general practice and hospital admissions for ambulatory care sensitive conditions: cross sectional study of routinely collected, person level data. BMJ. 2017;356(j84). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
