

Physiologic Assessment after Coronary Stent Implantation
- PMID: 33655719
- PMCID: PMC7925968
- DOI: 10.4070/kcj.2020.0548
Physiologic Assessment after Coronary Stent Implantation
Abstract
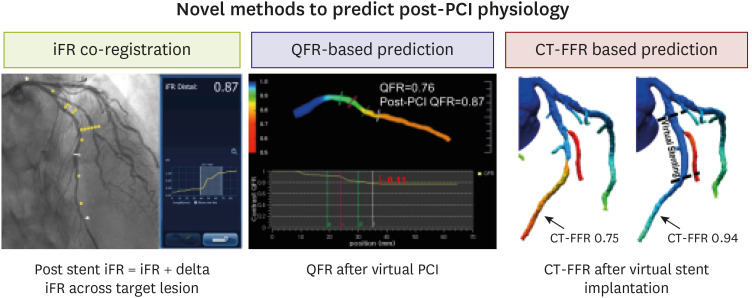
The presence of myocardial ischemia is a prerequisite for the benefit of coronary revascularization. In the cardiac catheterization laboratory, fractional flow reserve and non-hyperemic pressure ratios are used to define the ischemia-causing coronary stenosis, and several randomized studies showed the benefit of physiology-guided coronary revascularization. However, physiology-guided revascularization does not necessarily guarantee the relief of ischemia. Recent studies reported that residual ischemia might exist in up to 15-20% of cases after angiographically successful percutaneous coronary intervention (PCI). Therefore, post-PCI physiologic assessment is necessary for judging the appropriateness of PCI, detecting the lesions that may benefit from additional PCI, and risk stratification after PCI. This review will focus on the current evidence for post-PCI physiologic assessment, how to interpret these findings, and the future perspectives of physiologic assessment after PCI.
Keywords: Fractional flow reserve; Non-hyperemic pressure ratio; Outcomes; Percutaneous coronary intervention.
Copyright © 2021. The Korean Society of Cardiology.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures
Comment in
-
Non-Invasive Physiological Assessment after Coronary Stent Implantation.Korean Circ J. 2021 Jun;51(6):547-548. doi: 10.4070/kcj.2021.0156. Korean Circ J. 2021. PMID: 34085430 Free PMC article. No abstract available.
Similar articles
-
Blinded Physiological Assessment of Residual Ischemia After Successful Angiographic Percutaneous Coronary Intervention: The DEFINE PCI Study.JACC Cardiovasc Interv. 2019 Oct 28;12(20):1991-2001. doi: 10.1016/j.jcin.2019.05.054. JACC Cardiovasc Interv. 2019. PMID: 31648761
-
1-Year Outcomes of Blinded Physiological Assessment of Residual Ischemia After Successful PCI: DEFINE PCI Trial.JACC Cardiovasc Interv. 2022 Jan 10;15(1):52-61. doi: 10.1016/j.jcin.2021.09.042. JACC Cardiovasc Interv. 2022. PMID: 34991824 Clinical Trial.
-
Prognostic Implications of Post-Intervention Resting Pd/Pa and Fractional Flow Reserve in Patients With Stent Implantation.JACC Cardiovasc Interv. 2020 Aug 24;13(16):1920-1933. doi: 10.1016/j.jcin.2020.05.042. JACC Cardiovasc Interv. 2020. PMID: 32819481
-
Fractional flow reserve-guided coronary bypass surgery: should surgeons use it?Curr Opin Cardiol. 2013 Nov;28(6):654-60. doi: 10.1097/HCO.0b013e32836581a3. Curr Opin Cardiol. 2013. PMID: 24100651 Review.
-
Physiologic Assessment of Coronary Stenosis: Current Status and Future Directions.Curr Cardiol Rep. 2021 Jun 3;23(7):88. doi: 10.1007/s11886-021-01521-3. Curr Cardiol Rep. 2021. PMID: 34081223 Review.
Cited by
-
Effect of Coronary Disease Characteristics on Prognostic Relevance of Residual Ischemia After Stent Implantation.Front Cardiovasc Med. 2021 Dec 7;8:696756. doi: 10.3389/fcvm.2021.696756. eCollection 2021. Front Cardiovasc Med. 2021. PMID: 34950710 Free PMC article.
-
Coronary Physiology-Based Approaches for Plaque Vulnerability: Implications for Risk Prediction and Treatment Strategies.Korean Circ J. 2023 Sep;53(9):581-593. doi: 10.4070/kcj.2023.0117. Korean Circ J. 2023. PMID: 37653694 Free PMC article. Review.
-
Angiographic Findings and Post-Percutaneous Coronary Intervention Fractional Flow Reserve.JAMA Netw Open. 2024 Jun 3;7(6):e2418072. doi: 10.1001/jamanetworkopen.2024.18072. JAMA Netw Open. 2024. PMID: 38904958 Free PMC article.
-
Non-invasive vs. Invasive Functional Tests after Coronary Stent Implantation.Korean Circ J. 2021 Jun;51(6):549-550. doi: 10.4070/kcj.2021.1561. Korean Circ J. 2021. PMID: 34085427 Free PMC article. No abstract available.
-
Physiology- or Imaging-Guided Strategies for Intermediate Coronary Stenosis.JAMA Netw Open. 2024 Jan 2;7(1):e2350036. doi: 10.1001/jamanetworkopen.2023.50036. JAMA Netw Open. 2024. PMID: 38170524 Free PMC article.
References
-
- Hoole SP, Bambrough P. Recent advances in percutaneous coronary intervention. Heart. 2020;106:1380–1386. - PubMed
-
- Boden WE, O'Rourke RA, Teo KK, et al. Optimal medical therapy with or without PCI for stable coronary disease. N Engl J Med. 2007;356:1503–1516. - PubMed
-
- Shaw LJ, Berman DS, Maron DJ, et al. Optimal medical therapy with or without percutaneous coronary intervention to reduce ischemic burden: results from the clinical outcomes utilizing revascularization and aggressive drug evaluation (COURAGE) trial nuclear substudy. Circulation. 2008;117:1283–1291. - PubMed
-
- Neumann FJ, Sousa-Uva M, Ahlsson A, et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J. 2019;40:87–165. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
