

Digital Technology Interventions for Risk Factor Modification in Patients With Cardiovascular Disease: Systematic Review and Meta-analysis
- PMID: 33656444
- PMCID: PMC7970167
- DOI: 10.2196/21061
Digital Technology Interventions for Risk Factor Modification in Patients With Cardiovascular Disease: Systematic Review and Meta-analysis
Abstract
Background: Approximately 50% of cardiovascular disease (CVD) cases are attributable to lifestyle risk factors. Despite widespread education, personal knowledge, and efficacy, many individuals fail to adequately modify these risk factors, even after a cardiovascular event. Digital technology interventions have been suggested as a viable equivalent and potential alternative to conventional cardiac rehabilitation care centers. However, little is known about the clinical effectiveness of these technologies in bringing about behavioral changes in patients with CVD at an individual level.
Objective: The aim of this study is to identify and measure the effectiveness of digital technology (eg, mobile phones, the internet, software applications, wearables, etc) interventions in randomized controlled trials (RCTs) and determine which behavior change constructs are effective at achieving risk factor modification in patients with CVD.
Methods: This study is a systematic review and meta-analysis of RCTs designed according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analysis) statement standard. Mixed data from studies extracted from selected research databases and filtered for RCTs only were analyzed using quantitative methods. Outcome hypothesis testing was set at 95% CI and P=.05 for statistical significance.
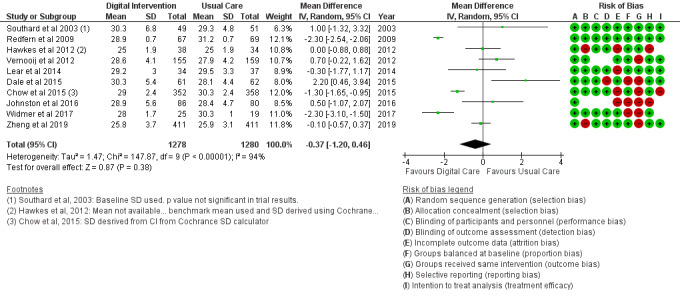
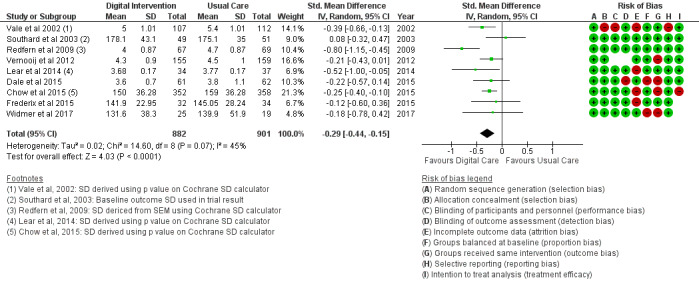
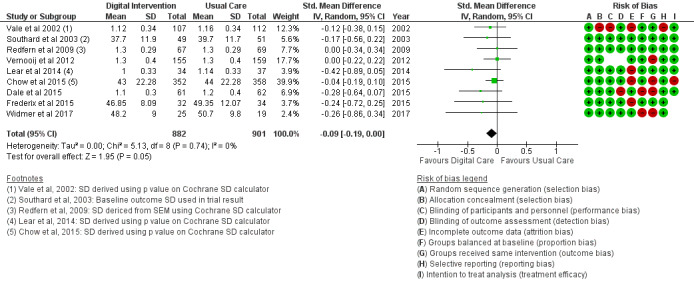
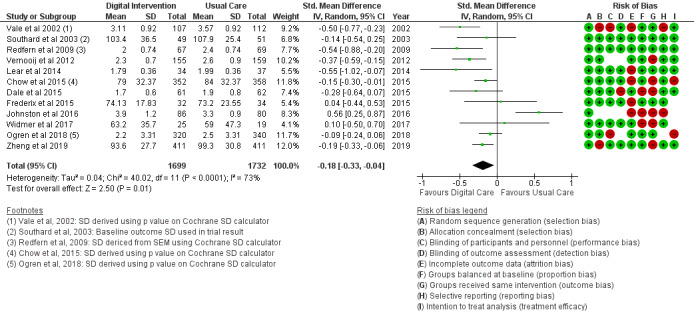
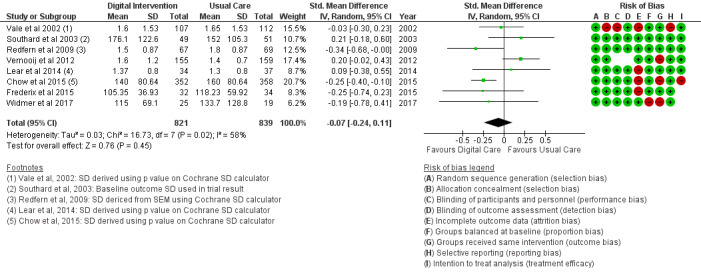
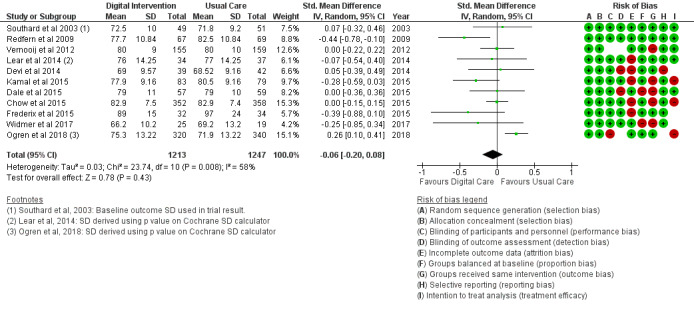
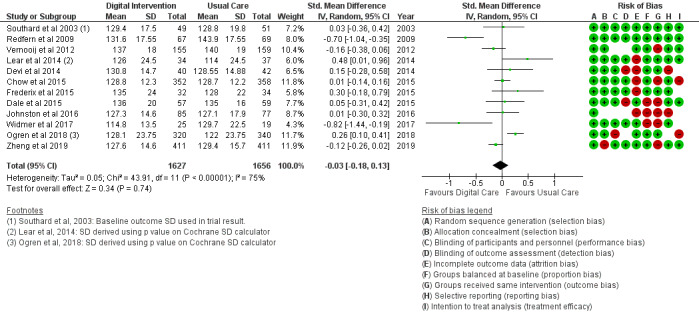
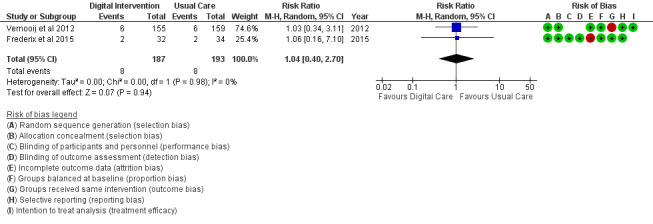
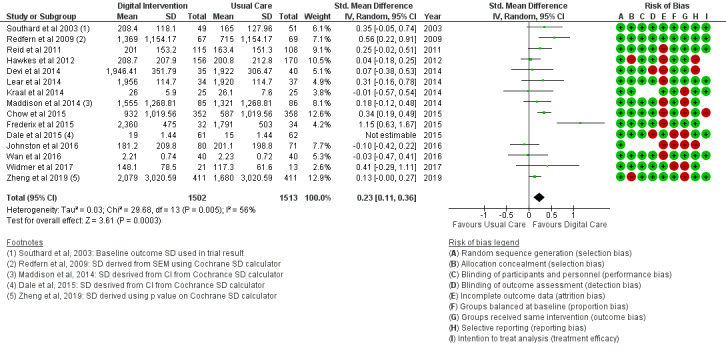
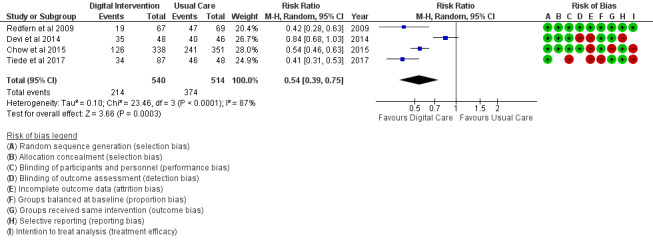
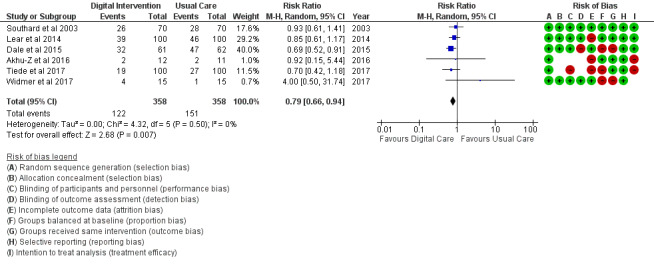
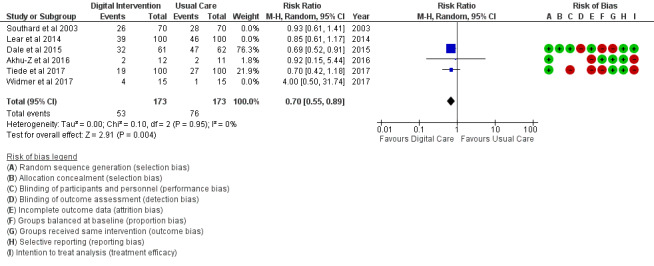
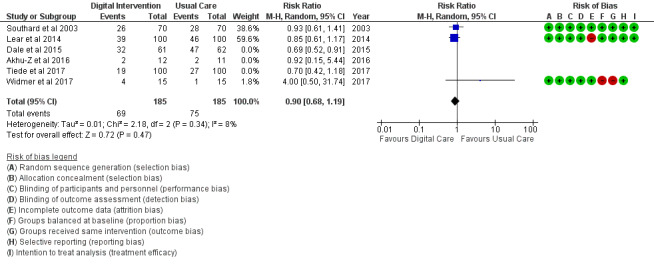
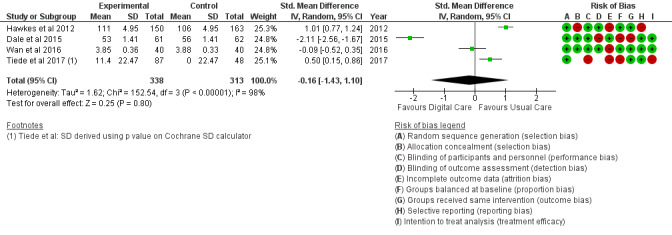
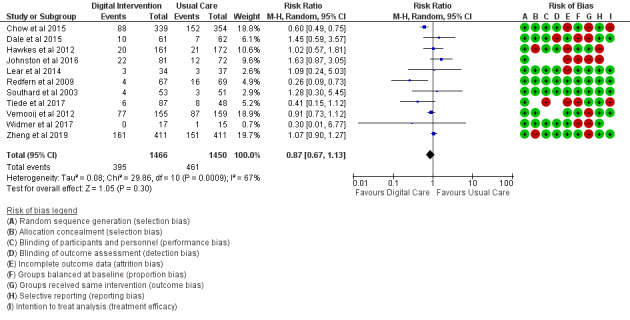
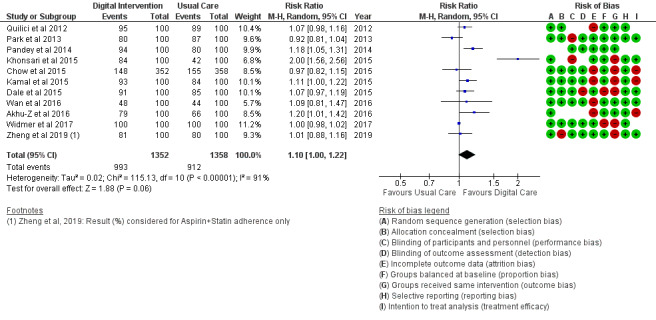
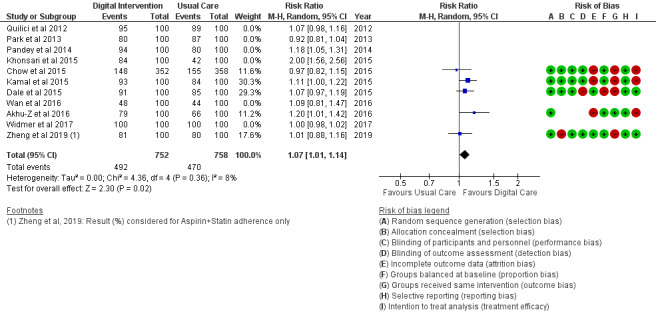
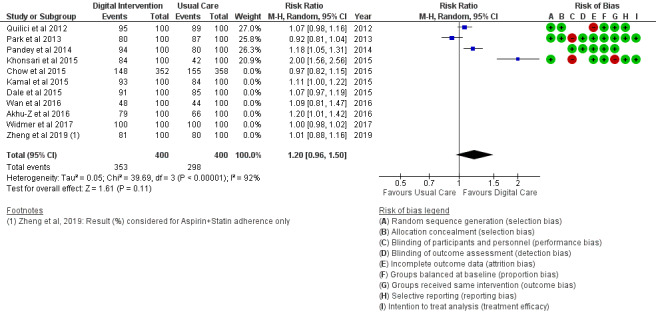
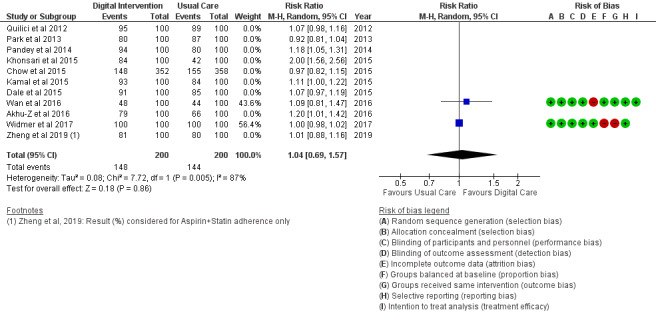
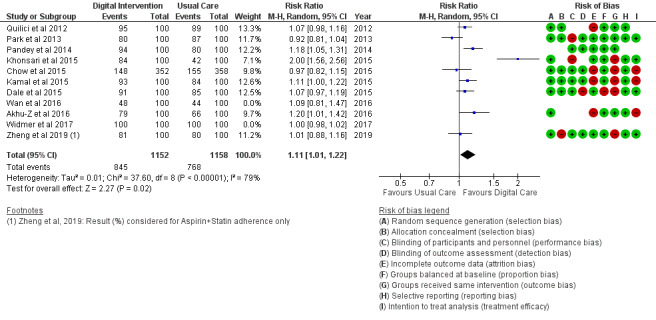
Results: Digital interventions were delivered using devices such as cell phones, smartphones, personal computers, and wearables coupled with technologies such as the internet, SMS, software applications, and mobile sensors. Behavioral change constructs such as cognition, follow-up, goal setting, record keeping, perceived benefit, persuasion, socialization, personalization, rewards and incentives, support, and self-management were used. The meta-analyzed effect estimates (mean difference [MD]; standard mean difference [SMD]; and risk ratio [RR]) calculated for outcomes showed benefits in total cholesterol SMD at -0.29 [-0.44, -0.15], P<.001; high-density lipoprotein SMD at -0.09 [-0.19, 0.00], P=.05; low-density lipoprotein SMD at -0.18 [-0.33, -0.04], P=.01; physical activity (PA) SMD at 0.23 [0.11, 0.36], P<.001; physical inactivity (sedentary) RR at 0.54 [0.39, 0.75], P<.001; and diet (food intake) RR at 0.79 [0.66, 0.94], P=.007. Initial effect estimates showed no significant benefit in body mass index (BMI) MD at -0.37 [-1.20, 0.46], P=.38; diastolic blood pressure (BP) SMD at -0.06 [-0.20, 0.08], P=.43; systolic BP SMD at -0.03 [-0.18, 0.13], P=.74; Hemoglobin A1C blood sugar (HbA1c) RR at 1.04 [0.40, 2.70], P=.94; alcohol intake SMD at -0.16 [-1.43, 1.10], P=.80; smoking RR at 0.87 [0.67, 1.13], P=.30; and medication adherence RR at 1.10 [1.00, 1.22], P=.06.
Conclusions: Digital interventions may improve healthy behavioral factors (PA, healthy diet, and medication adherence) and are even more potent when used to treat multiple behavioral outcomes (eg, medication adherence plus). However, they did not appear to reduce unhealthy behavioral factors (smoking, alcohol intake, and unhealthy diet) and clinical outcomes (BMI, triglycerides, diastolic and systolic BP, and HbA1c).
Keywords: behavior; cardiac rehabilitation; cardiovascular diseases; digital technologies; eHealth; mHealth; meta-analysis; mobile phone; risk factors; systematic review; telehealth.
©Adewale Samuel Akinosun, Rob Polson, Yohanca Diaz - Skeete, Johannes Hendrikus De Kock, Lucia Carragher, Stephen Leslie, Mark Grindle, Trish Gorely. Originally published in JMIR mHealth and uHealth (http://mhealth.jmir.org), 03.03.2021.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Cardiovascular diseases. World Health Organization. 2019. [2021-02-11]. https://www.who.int/health-topics/cardiovascular-diseases/
-
- Hospital Episode Statistics (HES) NHS Digital. 2017. [2021-02-11]. http://www.content.digital.nhs.uk/hes.
-
- Health diseases. British Heart Foundation. 2014. [2021-02-11]. https://www.bhf.org.uk/old-starts-with-your-heart/heart-diseases.
-
- Rocca HB, Fleischhacker L, Golubnitschaja O, Heemskerk F, Helms T, Hoedemakers T, Allianses SH, Jaarsma T, Kinkorova J, Ramaekers J, Ruff P, Schnur I, Vanoli E, Verdu J, Zippel-Schultz B. Challenges in personalised management of chronic diseases-heart failure as prominent example to advance the care process. EPMA J. 2015;7:2. doi: 10.1186/s13167-016-0051-9. http://europepmc.org/abstract/MED/26913090 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
