

Association of Long-term Use of Antihypertensive Medications With Late Outcomes Among Patients With Aortic Dissection
- PMID: 33656527
- PMCID: PMC7930924
- DOI: 10.1001/jamanetworkopen.2021.0469
Association of Long-term Use of Antihypertensive Medications With Late Outcomes Among Patients With Aortic Dissection
Abstract
Importance: The associations between long-term treatment of aortic dissection with various medications and late patient outcomes are poorly understood.
Objective: To compare late outcomes after long-term use of β-blockers, angiotensin-converting enzyme inhibitors (ACEIs), angiotensin receptor blockers (ARBs), or other antihypertensive medications (controls) among patients treated for aortic dissection.
Design, setting, and participants: This population-based retrospective cohort study using the National Health Insurance Research Database in Taiwan included 6978 adult patients with a first-ever aortic dissection who survived to hospital discharge during the period between January 1, 2001, and December 31, 2013, and who received during the first 90 days after discharge a prescription for an ACEI, ARB, β-blocker, or at least 1 other antihypertensive medication. Data analysis was conducted from July 2019 to June 2020.
Exposure: Long-term use of β-blockers, ACEIs, or ARBs, with use of other antihypertensive medications as a control.
Main outcomes and measures: The primary outcomes of interest were all-cause mortality, death due to aortic aneurism or dissection, later aortic operation, major adverse cardiac and cerebrovascular events, hospital readmission, and new-onset dialysis.
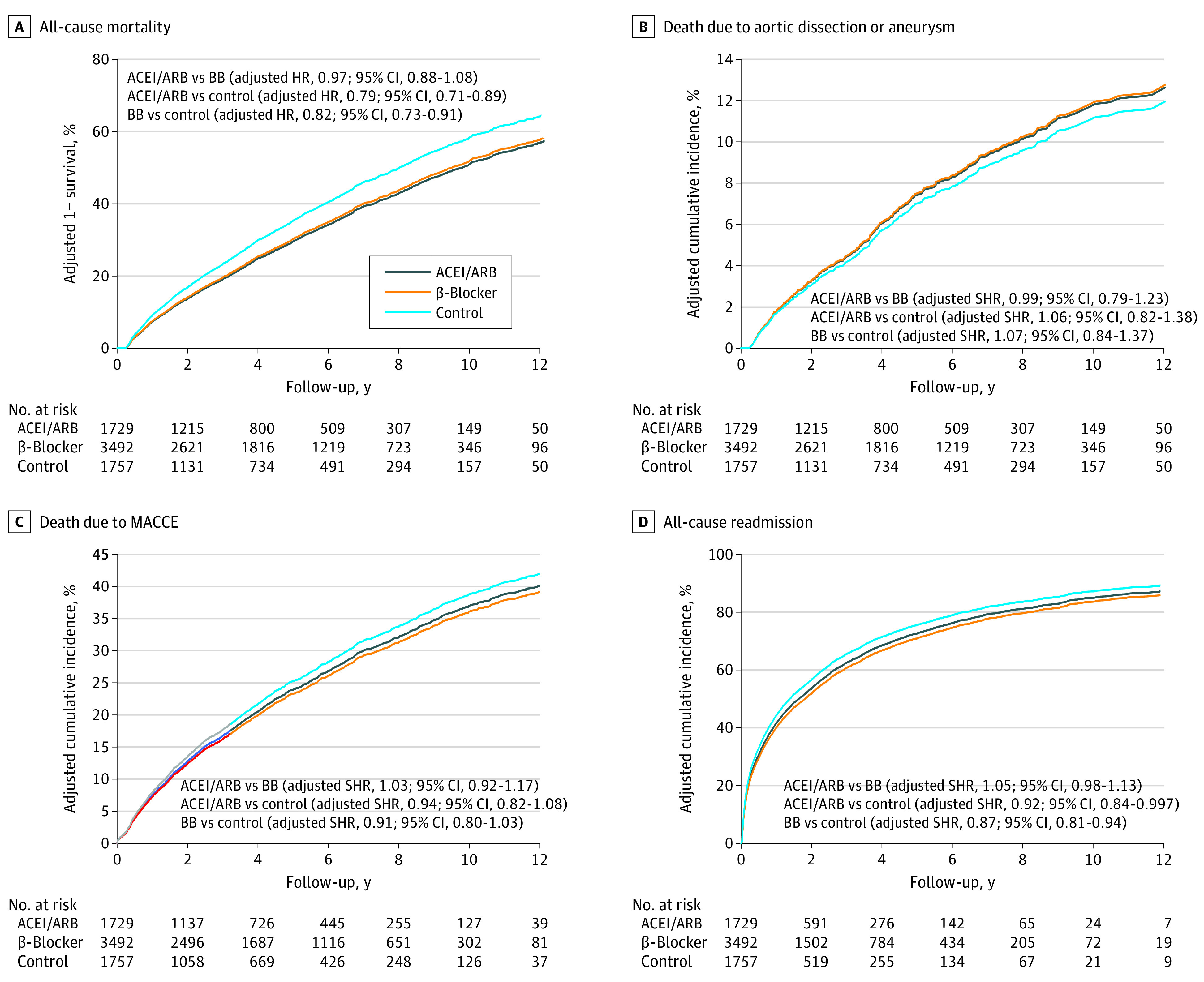
Results: Of 6978 total participants, 3492 received a β-blocker, 1729 received an ACEI or ARB, and 1757 received another antihypertension drug. Compared with patients in the other 2 groups, those in the β-blocker group were younger (mean [SD] age, 62.1 [13.9] years vs 68.7 [13.5] years for ACEIs or ARBs and 69.9 [13.8] years for controls) and comprised more male patients (2520 [72.2%] vs 1161 [67.1%] for ACEIs or ARBs and 1224 [69.7%] for controls). The prevalence of medicated hypertension was highest in the ACEI or ARB group (1039 patients [60.1%]), followed by the control group (896 patients [51.0%]), and was lowest in the β-blocker group (1577 patients [45.2%]). Patients who underwent surgery for type A aortic dissection were more likely to be prescribed β-blockers (1134 patients [32.5%]) than an ACEI or ARB (309 patients [17.9%]) or another antihypertension medication (376 patients [21.4%]). After adjusting for multiple propensity scores, there were no significant differences in any of the clinical characteristics among the 3 groups. No differences in the risks for all outcomes were observed between the ACEI or ARB and β-blocker groups. The risk of all-cause hospital readmission was significantly lower in the ACEI or ARB group (subdistribution hazard ratio [HR], 0.92; 95% CI, 0.84-0.997) and β-blocker group (subdistribution HR, 0.87; 95% CI, 0.81-0.94) than in the control group. Moreover, the risk of all-cause mortality was lower in the ACEI or ARB group (HR, 0.79; 95% CI, 0.71-0.89) and the β-blocker group (HR, 0.82; 95% CI, 0.73-0.91) than in the control group. In addition, the risk of all-cause mortality was lower in the ARB group than in the ACEI group (HR, 0.85; 95% CI, 0.76-0.95).
Conclusions and relevance: The use of β-blockers, ACEIs, or ARBs was associated with benefits in the long-term treatment of aortic dissection.
Conflict of interest statement
Figures


References
-
- Erbel R, Aboyans V, Boileau C, et al. ; ESC Committee for Practice Guidelines; The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC) . 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. Eur Heart J. 2014;35(41):2873-2926. doi: 10.1093/eurheartj/ehu281 - DOI - PubMed
-
- Hiratzka LF, Bakris GL, Beckman JA, et al. ; American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines; American Association for Thoracic Surgery; American College of Radiology; American Stroke Association; Society of Cardiovascular Anesthesiologists; Society for Cardiovascular Angiography and Interventions; Society of Interventional Radiology; Society of Thoracic Surgeons; Society for Vascular Medicine . 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with thoracic aortic disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. Circulation. 2010;121(13):e266-e369. doi: 10.1161/CIR0b013e3181d4739e - DOI - PubMed
-
- Suzuki T, Isselbacher EM, Nienaber CA, et al. ; IRAD Investigators . Type-selective benefits of medications in treatment of acute aortic dissection (from the International Registry of Acute Aortic Dissection [IRAD]). Am J Cardiol. 2012;109(1):122-127. doi: 10.1016/j.amjcard.2011.08.012 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
