

Changes in surgicaL behaviOrs dUring the CoviD-19 pandemic. The SICE CLOUD19 Study
- PMID: 33656697
- PMCID: PMC7926077
- DOI: 10.1007/s13304-021-01010-w
Changes in surgicaL behaviOrs dUring the CoviD-19 pandemic. The SICE CLOUD19 Study
Erratum in
-
Correction to: Changes in surgicaL behaviOrs dUring the CoviD-19 pandemic. The SICE CLOUD19 Study.Updates Surg. 2021 Aug;73(4):1597. doi: 10.1007/s13304-021-01072-w. Updates Surg. 2021. PMID: 33974192 Free PMC article. No abstract available.
Abstract
Background: The spread of the SARS-CoV2 virus, which causes COVID-19 disease, profoundly impacted the surgical community. Recommendations have been published to manage patients needing surgery during the COVID-19 pandemic. This survey, under the aegis of the Italian Society of Endoscopic Surgery, aims to analyze how Italian surgeons have changed their practice during the pandemic.
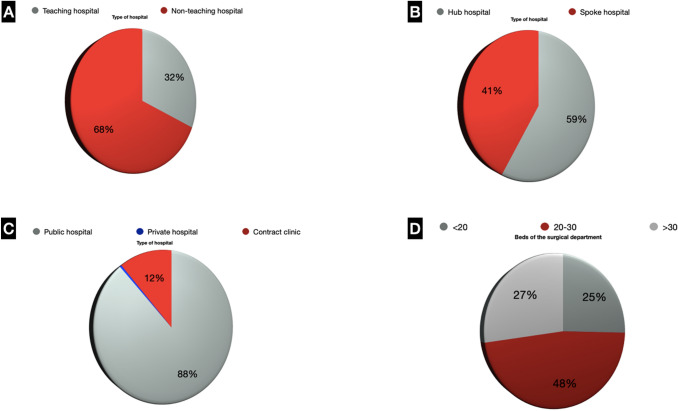
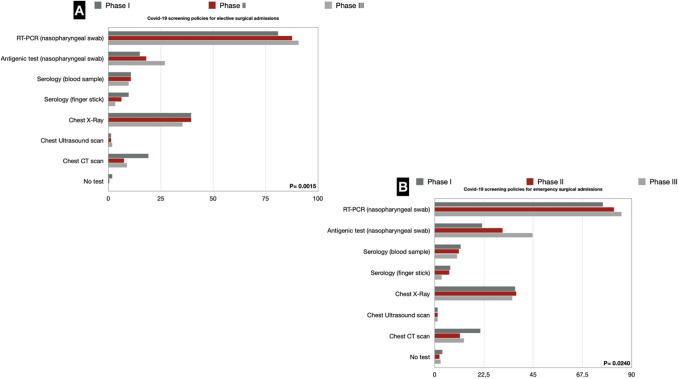
Methods: The authors designed an online survey that was circulated for completion to the Italian departments of general surgery registered in the Italian Ministry of Health database in December 2020. Questions were divided into three sections: hospital organization, screening policies, and safety profile of the surgical operation. The investigation periods were divided into the Italian pandemic phases I (March-May 2020), II (June-September 2020), and III (October-December 2020).
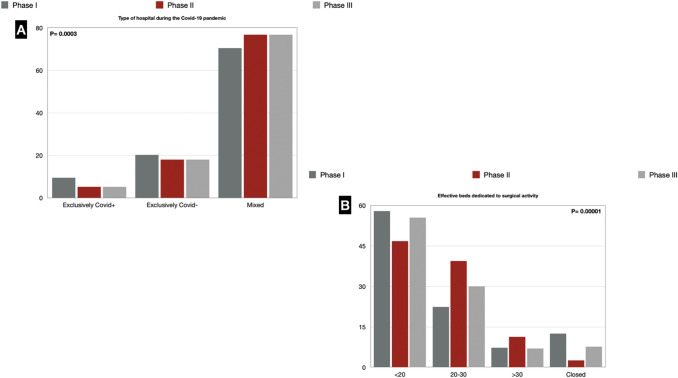
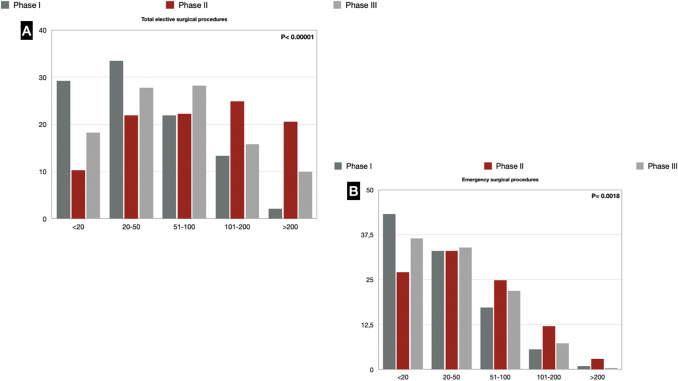
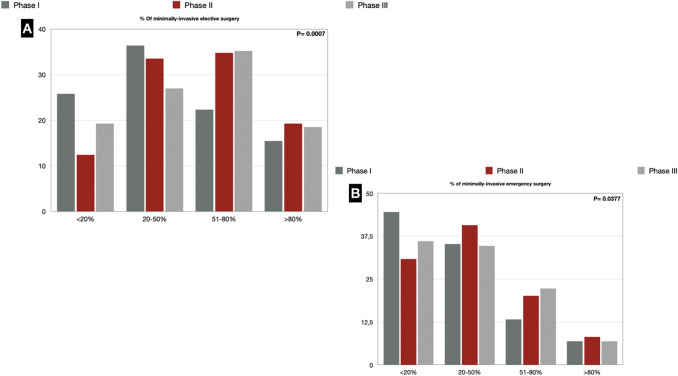
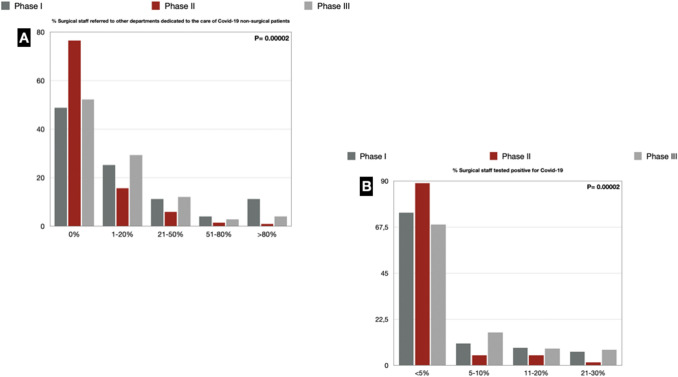
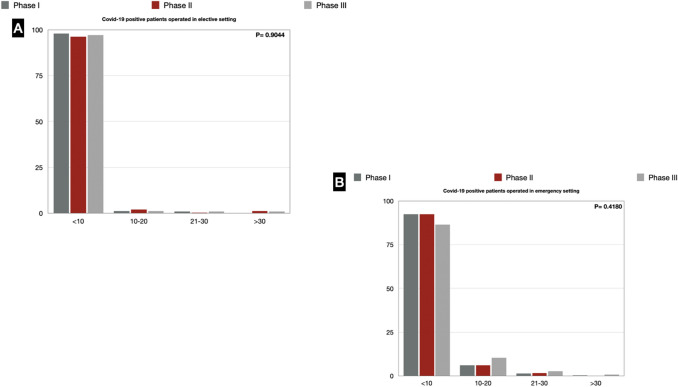
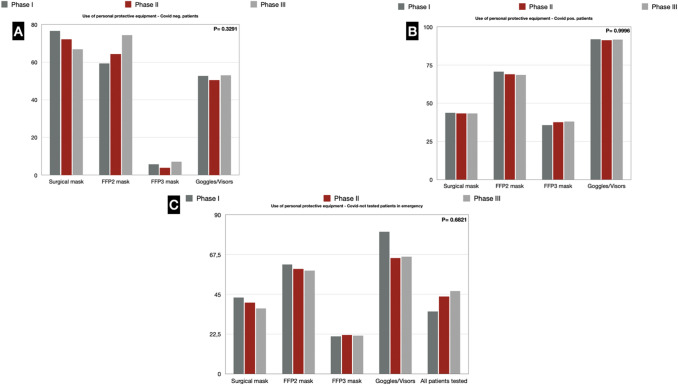
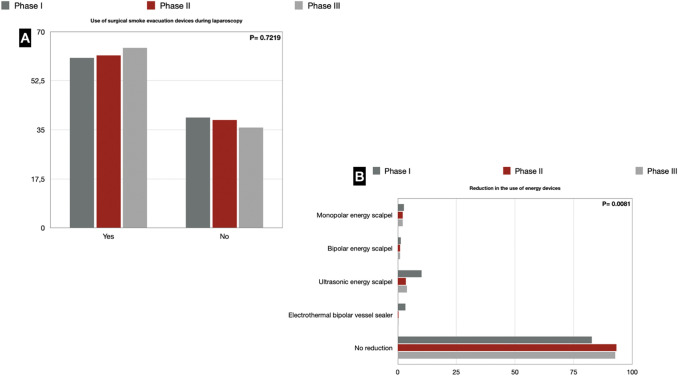
Results: Of 447 invited departments, 226 answered the survey. Most hospitals were treating both COVID-19-positive and -negative patients. The reduction in effective beds dedicated to surgical activity was significant, affecting 59% of the responding units. 12.4% of the respondents in phase I, 2.6% in phase II, and 7.7% in phase III reported that their surgical unit had been closed. 51.4%, 23.5%, and 47.8% of the respondents had at least one colleague reassigned to non-surgical COVID-19 activities during the three phases. There has been a reduction in elective (> 200 procedures: 2.1%, 20.6% and 9.9% in the three phases, respectively) and emergency (< 20 procedures: 43.3%, 27.1%, 36.5% in the three phases, respectively) surgical activity. The use of laparoscopy also had a setback in phase I (25.8% performed less than 20% of elective procedures through laparoscopy). 60.6% of the respondents used a smoke evacuation device during laparoscopy in phase I, 61.6% in phase II, and 64.2% in phase III. Almost all responders (82.8% vs. 93.2% vs. 92.7%) in each analyzed period did not modify or reduce the use of high-energy devices.
Conclusion: This survey offers three faithful snapshots of how the surgical community has reacted to the COVID-19 pandemic during its three phases. The significant reduction in surgical activity indicates that better health policies and more evidence-based guidelines are needed to make up for lost time and surgery not performed during the pandemic.
Keywords: COVID-19; Elective surgery; Emergency surgery; Laparoscopic surgery; Survey.
Conflict of interest statement
The authors have no relevant financial or non-financial interests to disclose.
Figures
Comment in
-
Commentary: Changes in Oral Health Policies and Guidelines During the COVID-19 Pandemic.Front Oral Health. 2021 Jul 8;2:718538. doi: 10.3389/froh.2021.718538. eCollection 2021. Front Oral Health. 2021. PMID: 35048044 Free PMC article. No abstract available.
References
-
- W. H. O. (OMS), “COVID-19 Weekly Epidemiological Update,” no. November, p. 1;4, 2020.
-
- Bellato V, Konishi T, Pellino G, An Y, Piciocchi A, Sensi B, Siragusa L, Khanna K, Pirozzi BM, Franceschilli M, Campanelli M, Efetov S, Sica GS, S-COVID Collaborative Group Screening policies, preventive measures and in-hospital infection of COVID-19 in global surgical practices. J Glob Health. 2020;10(2):020507. doi: 10.7189/jogh.10.020507. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
