

Associations with antibiotic prescribing for acute exacerbation of COPD in primary care: secondary analysis of a randomised controlled trial
- PMID: 33657007
- PMCID: PMC8007268
- DOI: 10.3399/BJGP.2020.0823
Associations with antibiotic prescribing for acute exacerbation of COPD in primary care: secondary analysis of a randomised controlled trial
Abstract
Background: C-reactive protein (CRP) point-of-care testing can reduce antibiotic use in patients with acute exacerbation of chronic obstructive pulmonary disease (AECOPD) in primary care, without compromising patient care. Further safe reductions may be possible.
Aim: To investigate the associations between presenting features and antibiotic prescribing in patients with AECOPD in primary care.
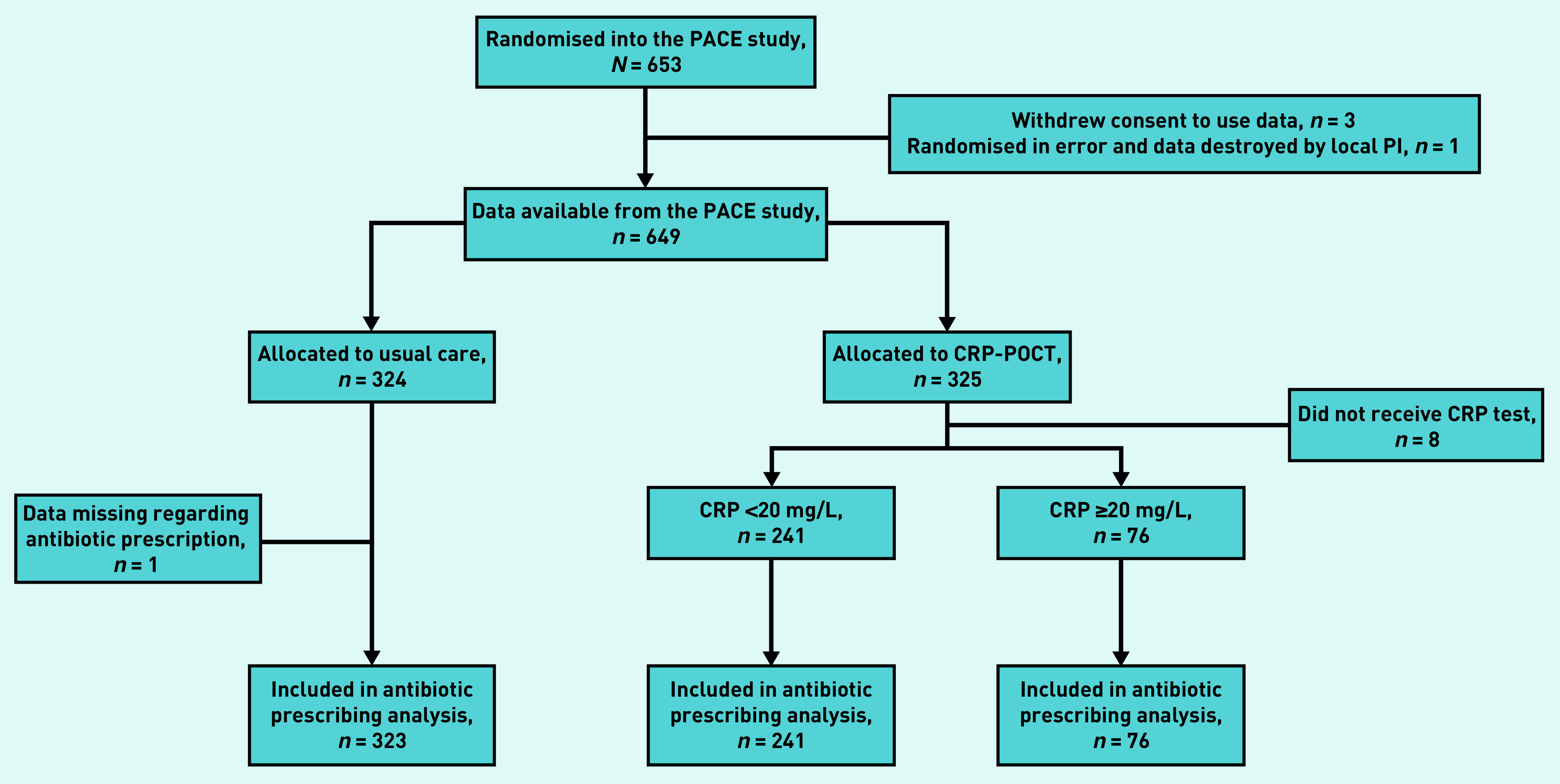
Design and setting: Secondary analysis of a randomised controlled trial of participants presenting with AECOPD in primary care (the PACE trial).
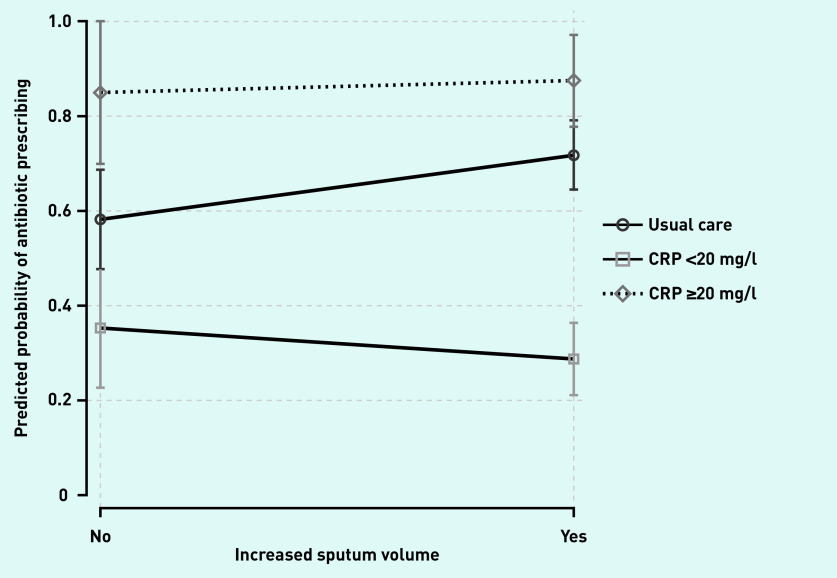
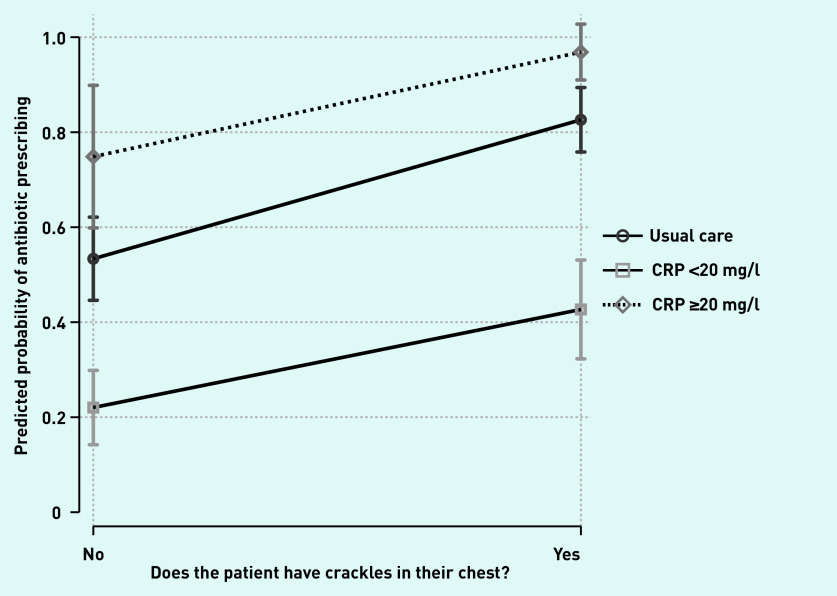
Method: Clinicians collected participants' demographic features, comorbid illnesses, clinical signs, and symptoms. Antibiotic prescribing decisions were made after participants were randomised to receive a point-of-care CRP measurement or usual care. Multivariable regression models were fitted to explore the association between patient and clinical features and antibiotic prescribing, and extended to further explore any interactions with CRP measurement category (CRP not measured, CRP <20 mg/l, or CRP ≥20 mg/l).
Results: A total of 649 participants from 86 general practices across England and Wales were included. Odds of antibiotic prescribing were higher in the presence of clinician-recorded crackles (adjusted odds ratio [AOR] = 5.22, 95% confidence interval [CI] = 3.24 to 8.41), wheeze (AOR = 1.64, 95% CI = 1.07 to 2.52), diminished vesicular breathing (AOR = 2.95, 95% CI = 1.70 to 5.10), or clinician-reported evidence of consolidation (AOR = 34.40, 95% CI = 2.84 to 417.27). Increased age was associated with lower odds of antibiotic prescribing (AOR per additional year increase = 0.98, 95% CI = 0.95 to 1.00), as was the presence of heart failure (AOR = 0.32, 95% CI = 0.12 to 0.85).
Conclusion: Several demographic features and clinical signs and symptoms are associated with antibiotic prescribing in AECOPD. Diagnostic and prognostic value of these features may help identify further safe reductions.
Keywords: C-reactive protein; COPD; antibiotics; primary care; randomised controlled trial.
© The Authors.
Figures
References
-
- World Health Organization The top 10 causes of death. 2020 https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed 18 Feb 2021).
-
- Nacul L, Soljak M, Samarasundera E, et al. COPD in England: a comparison of expected, model-based prevalence and observed prevalence from general practice data. J Public Health (Oxf) 2011;33(1):108–116. - PubMed
-
- Llor C, Bjerrum L, Munck A, et al. Predictors for antibiotic prescribing in patients with exacerbations of COPD in general practice. Ther Adv Respir Dis. 2013;7(3):131–137. - PubMed
-
- Celli BR, Barnes PJ. Exacerbations of chronic obstructive pulmonary disease. Eur Respir J. 2007;29(6):1224–1238. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous