

Trends in heart failure-related cardiovascular mortality in rural versus urban United States counties, 2011-2018: A cross-sectional study
- PMID: 33657143
- PMCID: PMC7928489
- DOI: 10.1371/journal.pone.0246813
Trends in heart failure-related cardiovascular mortality in rural versus urban United States counties, 2011-2018: A cross-sectional study
Abstract
Background: Adults in rural counties in the United States (US) experience higher rates broadly of cardiovascular disease (CVD) compared with adults in urban counties. Mortality rates specifically due to heart failure (HF) have increased since 2011, but estimates of heterogeneity at the county-level in HF-related mortality have not been produced. The objectives of this study were 1) to quantify nationwide trends by rural-urban designation and 2) examine county-level factors associated with rural-urban differences in HF-related mortality rates.
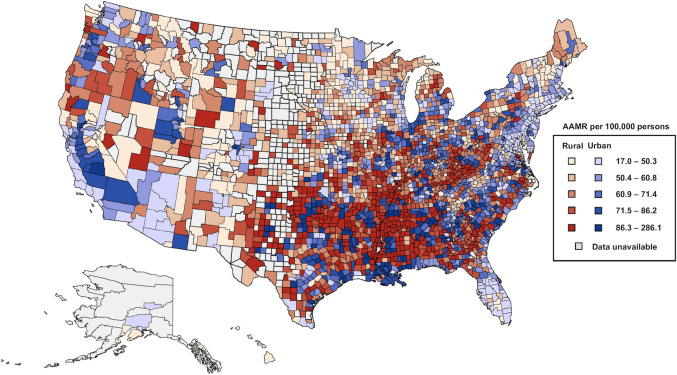
Methods and findings: We queried CDC WONDER to identify HF deaths between 2011-2018 defined as CVD (I00-78) as the underlying cause of death and HF (I50) as a contributing cause of death. First, we calculated national age-adjusted mortality rates (AAMR) and examined trends stratified by rural-urban status (defined using 2013 NCHS Urban-Rural Classification Scheme), age (35-64 and 65-84 years), and race-sex subgroups per year. Second, we combined all deaths from 2011-2018 and estimated incidence rate ratios (IRR) in HF-related mortality for rural versus urban counties using multivariable negative binomial regression models with adjustment for demographic and socioeconomic characteristics, risk factor prevalence, and physician density. Between 2011-2018, 162,314 and 580,305 HF-related deaths occurred in rural and urban counties, respectively. AAMRs were consistently higher for residents in rural compared with urban counties (73.2 [95% CI: 72.2-74.2] vs. 57.2 [56.8-57.6] in 2018, respectively). The highest AAMR was observed in rural Black men (131.1 [123.3-138.9] in 2018) with greatest increases in HF-related mortality in those 35-64 years (+6.1%/year). The rural-urban IRR persisted among both younger (1.10 [1.04-1.16]) and older adults (1.04 [1.02-1.07]) after adjustment for county-level factors. Main limitations included lack of individual-level data and county dropout due to low event rates (<20).
Conclusions: Differences in county-level factors may account for a significant amount of the observed variation in HF-related mortality between rural and urban counties. Efforts to reduce the rural-urban disparity in HF-related mortality rates will likely require diverse public health and clinical interventions targeting the underlying causes of this disparity.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures



Similar articles
-
Assessment of Racial Disparities in Mortality Rates Among Older Adults Living in US Rural vs Urban Counties From 1968 to 2016.JAMA Netw Open. 2020 Aug 3;3(8):e2012241. doi: 10.1001/jamanetworkopen.2020.12241. JAMA Netw Open. 2020. PMID: 32744631 Free PMC article.
-
Potentially Excess Deaths from the Five Leading Causes of Death in Metropolitan and Nonmetropolitan Counties - United States, 2010-2017.MMWR Surveill Summ. 2019 Nov 8;68(10):1-11. doi: 10.15585/mmwr.ss6810a1. MMWR Surveill Summ. 2019. PMID: 31697657
-
Preventable Premature Deaths from the Five Leading Causes of Death in Nonmetropolitan and Metropolitan Counties, United States, 2010-2022.MMWR Surveill Summ. 2024 May 2;73(2):1-11. doi: 10.15585/mmwr.ss7302a1. MMWR Surveill Summ. 2024. PMID: 38687830 Free PMC article.
-
Geographic access to cardiac rehabilitation and cardiovascular disease outcomes: A study of rural United States counties.Curr Probl Cardiol. 2024 Sep;49(9):102740. doi: 10.1016/j.cpcardiol.2024.102740. Epub 2024 Jul 5. Curr Probl Cardiol. 2024. PMID: 38972468 Review.
-
Shifting trends and disparities in colorectal cancer and heart failure-related mortality in the United States: A two-decade retrospective analysis.Curr Probl Cardiol. 2025 Jun;50(6):103034. doi: 10.1016/j.cpcardiol.2025.103034. Epub 2025 Mar 20. Curr Probl Cardiol. 2025. PMID: 40120869 Review.
Cited by
-
Rurality, Cardiovascular Risk Factors, and Early Cardiovascular Disease among Childhood, Adolescent, and Young Adult Cancer Survivors.Res Sq [Preprint]. 2024 Apr 1:rs.3.rs-4139837. doi: 10.21203/rs.3.rs-4139837/v1. Res Sq. 2024. Update in: J Adolesc Young Adult Oncol. 2025 Mar 25. doi: 10.1089/jayao.2024.0151. PMID: 38645102 Free PMC article. Updated. Preprint.
-
Demographic trends and disparities in mortality related to coexisting heart failure and diabetes mellitus among older adults in the United States between 1999 and 2020: A retrospective population-based cohort study from the CDC WONDER database.Int J Cardiol Cardiovasc Risk Prev. 2024 Aug 24;23:200326. doi: 10.1016/j.ijcrp.2024.200326. eCollection 2024 Dec. Int J Cardiol Cardiovasc Risk Prev. 2024. PMID: 39282605 Free PMC article.
-
"We Are the Champions": Victory for VICTORIA Trial.JACC Heart Fail. 2023 Sep;11(9):1258-1261. doi: 10.1016/j.jchf.2023.06.026. Epub 2023 Aug 9. JACC Heart Fail. 2023. PMID: 37565980 Free PMC article. No abstract available.
-
Demographic trends of cardiorenal and heart failure deaths in the United States, 2011-2020.PLoS One. 2024 May 29;19(5):e0302203. doi: 10.1371/journal.pone.0302203. eCollection 2024. PLoS One. 2024. PMID: 38809898 Free PMC article.
-
Rural, Large Town, and Urban Differences in Optimal Subspecialty Follow-up and Survivorship Care Plan Documentation among Childhood Cancer Survivors.Cancer Epidemiol Biomarkers Prev. 2023 May 1;32(5):634-641. doi: 10.1158/1055-9965.EPI-22-0966. Cancer Epidemiol Biomarkers Prev. 2023. PMID: 36827210 Free PMC article.
References
-
- Roth AR, Denney JT, Amiri S, Amram O. Characteristics of place and the rural disadvantage in deaths from highly preventable causes. Social Science & Medicine. 2020;245:112689. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
