

Posttransplant cyclophosphamide is associated with increased cytomegalovirus infection: a CIBMTR analysis
- PMID: 33657221
- PMCID: PMC8351903
- DOI: 10.1182/blood.2020009362
Posttransplant cyclophosphamide is associated with increased cytomegalovirus infection: a CIBMTR analysis
Abstract
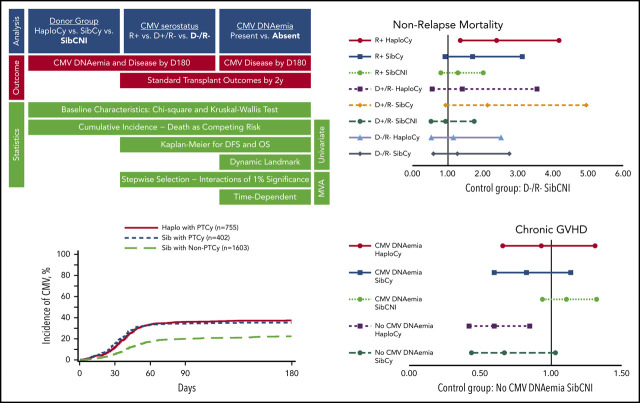
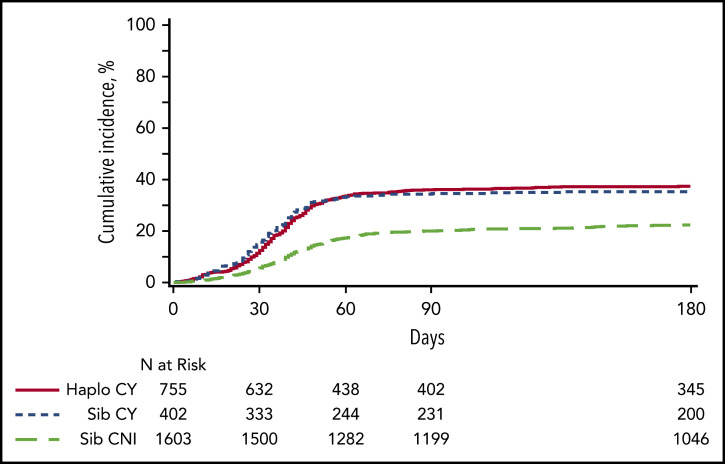
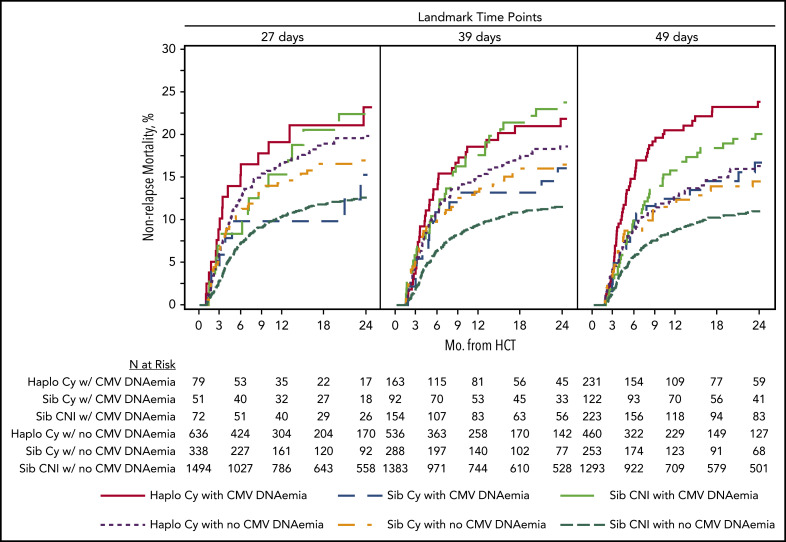
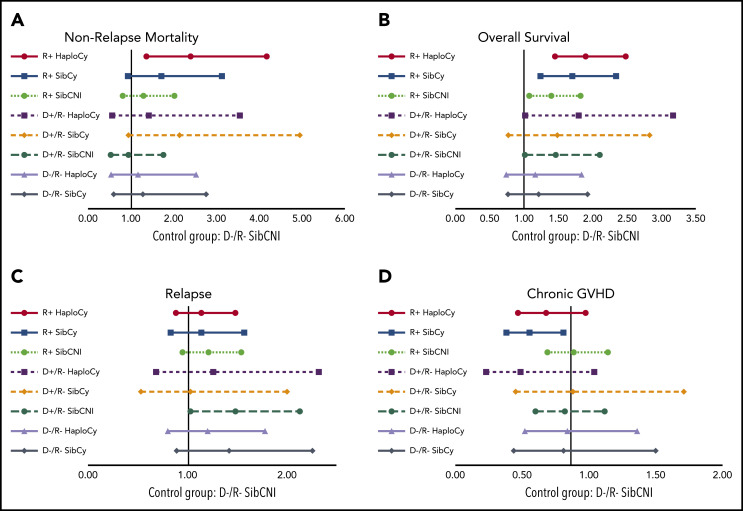
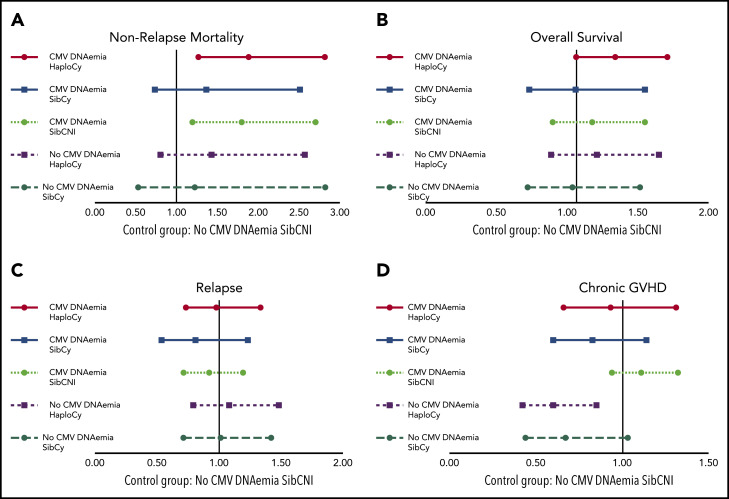
Prior studies suggest increased cytomegalovirus (CMV) infection after haploidentical donor transplantation with posttransplant cyclophosphamide (HaploCy). The role of allograft source and posttransplant cyclophosphamide (PTCy) in CMV infection is unclear. We analyzed the effect of graft source and PTCy on incidence of CMV infection, and effects of serostatus and CMV infection on transplant outcomes. We examined patients reported to the Center for International Blood and Marrow Transplantation Research between 2012 and 2017 who had received HaploCy (n = 757), matched related (Sib) with PTCy (SibCy, n = 403), or Sib with calcineurin inhibitor-based prophylaxis (SibCNI, n = 1605). Cumulative incidences of CMV infection by day 180 were 42%, 37%, and 23%, respectively (P < .001). CMV disease was statistically comparable. CMV infection risk was highest for CMV-seropositive recipients (R+), but significantly higher in PTCy recipients regardless of donor (HaploCy [n = 545]: hazard ratio [HR], 50.3; SibCy [n = 279]: HR, 47.7; SibCNI [n = 1065]: HR, 24.4; P < .001). D+/R- patients also had increased risk for CMV infection. Among R+ or those developing CMV infection, HaploCy had worse overall survival and nonrelapse mortality. Relapse was unaffected by CMV infection or serostatus. PTCy was associated with lower chronic graft-versus-host disease (GVHD) overall, but CMV infection in PTCy recipients was associated with higher chronic GVHD (P = .006). PTCy, regardless of donor, is associated with higher incidence of CMV infection, augmenting the risk of seropositivity. Additionally, CMV infection may negate the chronic GVHD protection of PTCy. This study supports aggressive prevention strategies in all receiving PTCy.
Keywords: CIMBTR; CMV; MARROW AND STEM CELL TRANSPLANTATION; haploidentical; organ specific toxicity: infectious; outcomes; posttransplant cyclophosphamide.
Figures
Comment in
-
Expect the unexpected.Blood. 2021 Jun 10;137(23):3163-3164. doi: 10.1182/blood.2021011368. Blood. 2021. PMID: 34110401 Free PMC article. No abstract available.
References
-
- Nishihori T, El-Asmar J, Aljurf M, Kharfan-Dabaja MA. Therapeutic strategies for cytomegalovirus in allogeneic hematopoietic cell transplantation. Immunotherapy. 2015;7(10):1059-1071. - PubMed
-
- Ariza-Heredia EJ, Nesher L, Chemaly RF. Cytomegalovirus diseases after hematopoietic stem cell transplantation: a mini-review. Cancer Lett. 2014;342(1):1-8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U01 AI126612/AI/NIAID NIH HHS/United States
- U01 HL128568/HL/NHLBI NIH HHS/United States
- P30 CA008748/CA/NCI NIH HHS/United States
- R01 HL129472/HL/NHLBI NIH HHS/United States
- P01 CA111412/CA/NCI NIH HHS/United States
- R01 CA215134/CA/NCI NIH HHS/United States
- R01 HL131731/HL/NHLBI NIH HHS/United States
- R01 HL126589/HL/NHLBI NIH HHS/United States
- R01 CA152108/CA/NCI NIH HHS/United States
- U24 CA076518/CA/NCI NIH HHS/United States
- U24 HL138660/HL/NHLBI NIH HHS/United States
- U01 AI069197/AI/NIAID NIH HHS/United States
- R01 CA231141/CA/NCI NIH HHS/United States
- R01 CA218285/CA/NCI NIH HHS/United States
- R01 HL130388/HL/NHLBI NIH HHS/United States
- R25 CA190190/CA/NCI NIH HHS/United States
- R01 AI128775/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
