

Misdiagnosis and diagnostic pitfalls of chronic inflammatory demyelinating polyradiculoneuropathy
- PMID: 33657260
- PMCID: PMC8252611
- DOI: 10.1111/ene.14796
Misdiagnosis and diagnostic pitfalls of chronic inflammatory demyelinating polyradiculoneuropathy
Abstract
Background and purpose: The aim of this study was to determine the frequency of over- and underdiagnosis of chronic inflammatory demyelinating polyradiculoneuropathy (CIDP) and to identify related diagnostic pitfalls.
Methods: We conducted a retrospective study in Dutch patients referred to the Erasmus University Medical Centre Rotterdam between 2011 and 2017 with either a diagnosis of CIDP or another diagnosis that was revised to CIDP. We used the European Federation of Neurological Societies/Peripheral Nerve Society (EFNS/PNS) 2010 diagnostic criteria for CIDP to classify patients into three groups: overdiagnosis, underdiagnosis, or confirmed diagnosis of CIDP. Clinical and laboratory features and treatment history were compared between groups.
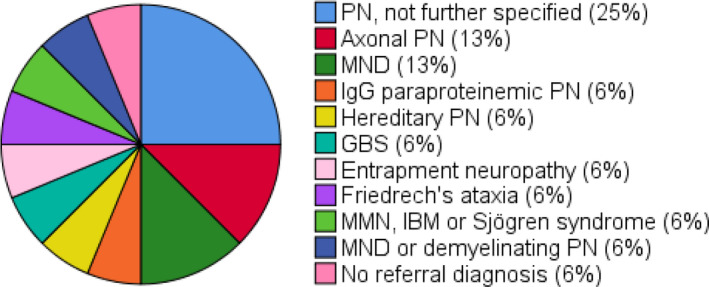
Results: A referral diagnosis of CIDP was revised in 32% of patients (31/96; overdiagnosis). Of 81 patients diagnosed with CIDP, 16 (20%) were referred with another diagnosis (underdiagnosis). In the overdiagnosed patients, 20% of muscle weakness was asymmetric, 48% lacked proximal muscle weakness, 29% only had distal muscle weakness, 65% did not fulfil the electrodiagnostic criteria for CIDP, 74% had an elevated cerebrospinal fluid (CSF) protein level, and 97% had another type of neuropathy. In the underdiagnosed patients, all had proximal muscle weakness, 50% had a clinically atypical CIDP, all fulfilled the electrodiagnostic criteria for CIDP, and 25% had an increased CSF protein level.
Conclusion: Over- and underdiagnosis of CIDP is common. Diagnostic pitfalls include lack of attention to proximal muscle weakness as a diagnostic hallmark of CIDP, insufficient recognition of clinical atypical phenotypes, overreliance on CSF protein levels, misinterpretation of nerve conduction studies and poor adherence to electrodiagnostic criteria, and failure to exclude other causes of polyneuropathy.
Keywords: CIDP; cerebrospinal fluid; chronic inflammatory demyelinating polyradiculoneuropathy; diagnostic errors; overdiagnosis; peripheral nervous system diseases; underdiagnosis.
© 2021 The Authors. European Journal of Neurology published by John Wiley & Sons Ltd on behalf of European Academy of Neurology.
Conflict of interest statement
Merel C. Broers and Hester F. Lingsma report grants from the Dutch Prinses Beatrix Spierfonds, during the conduct of the study. Carina Bunschoten, Judith Drenthen, Tiago A. O. Beck and Esther Brusse report no disclosures. Jeffrey A. Allen reports consultations with Akcea, Alexion, Argenx, Momenta, CSL Behring, Grifols and Biotest, outside the submitted work. Richard A. Lewis reports Consulting fees from Argenx, CSL Behring, Biotest, Annexon, Pharnext, Momenta, Pfizer, Sanofi and Takeda, and speaker honoraria for Akcea, Alnylam, CSL Behring and Medschape, outside the submitted work. Pieter A. van Doorn reports fees from Octapharma, Kedrion, CSL Behring, Grifols and Hansa (all fees to departmental research fund), grants from Dutch Prinses Beatrix Spierfonds, Sanquin, Takeda, Baxalta, Shire and Grifols, outside the submitted work. Bart C. Jacobs reports grants from the Dutch Prinses Beatrix Spierfond, during the conduct of the study, and grants from the Dutch Prinses Beatrix Spierfonds, Horizon 2020, GBS‐CIDP Foundation International, Baxalta, Grifols, CSL Behring, Annexon and Hansa Biopharma, outside the submitted work.
Figures


References
-
- Bunschoten C, Jacobs BC, Van den Bergh PYK, Cornblath DR, van Doorn PA. Progress in diagnosis and treatment of chronic inflammatory demyelinating polyradiculoneuropathy. Lancet Neurol. 2019;18(8):784‐794. - PubMed
-
- Neligan A, Reilly MM, Lunn MP. CIDP: mimics and chameleons. Pract Neurol. 2014;14(6):399‐408. - PubMed
-
- Allen JA, Lewis RA. CIDP diagnostic pitfalls and perception of treatment benefit. Neurology. 2015;85(6):498‐504. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
