

Diffuse Large B-Cell Lymphoma
- PMID: 33657296
- PMCID: PMC8377611
- DOI: 10.1056/NEJMra2027612
Diffuse Large B-Cell Lymphoma
Abstract
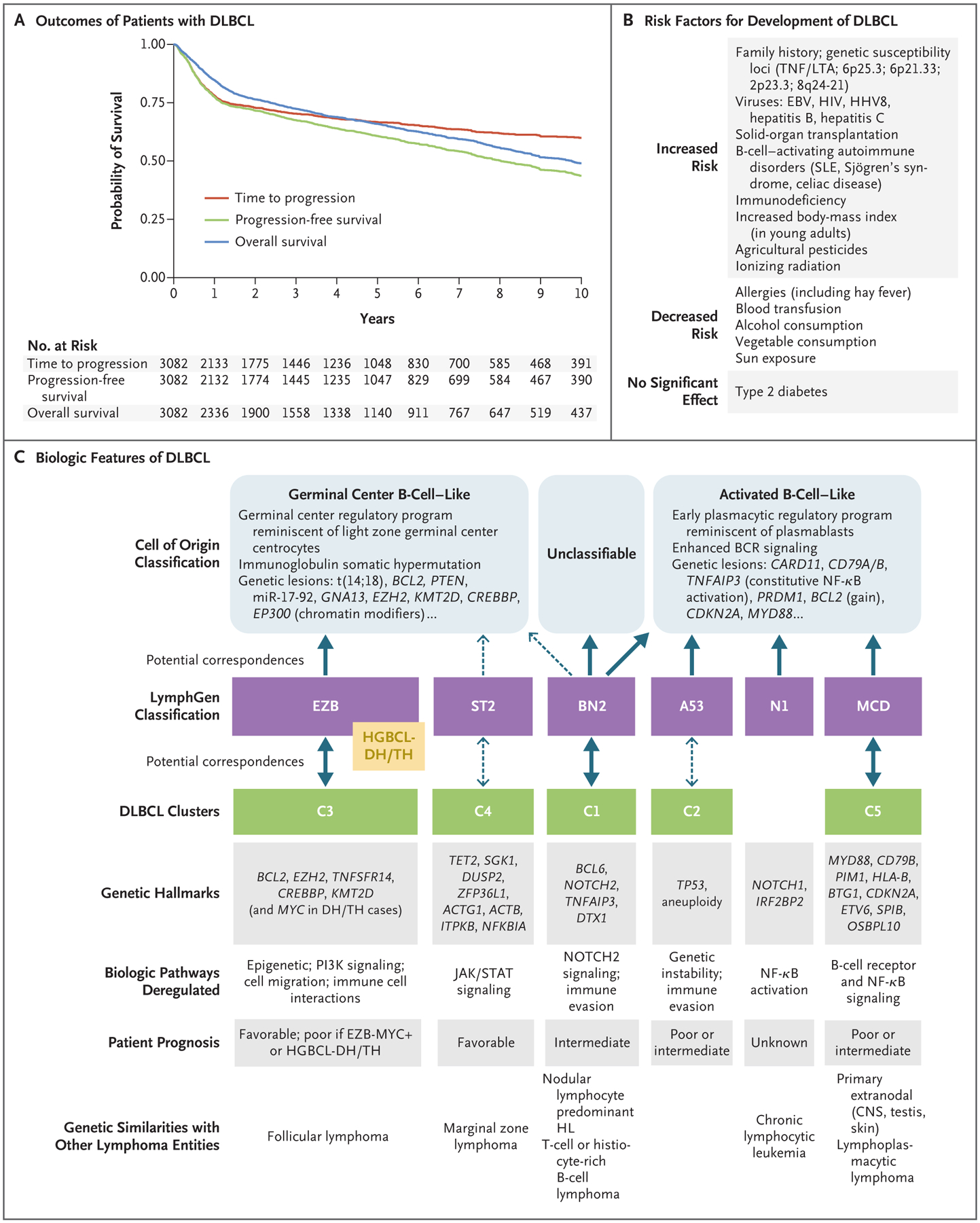
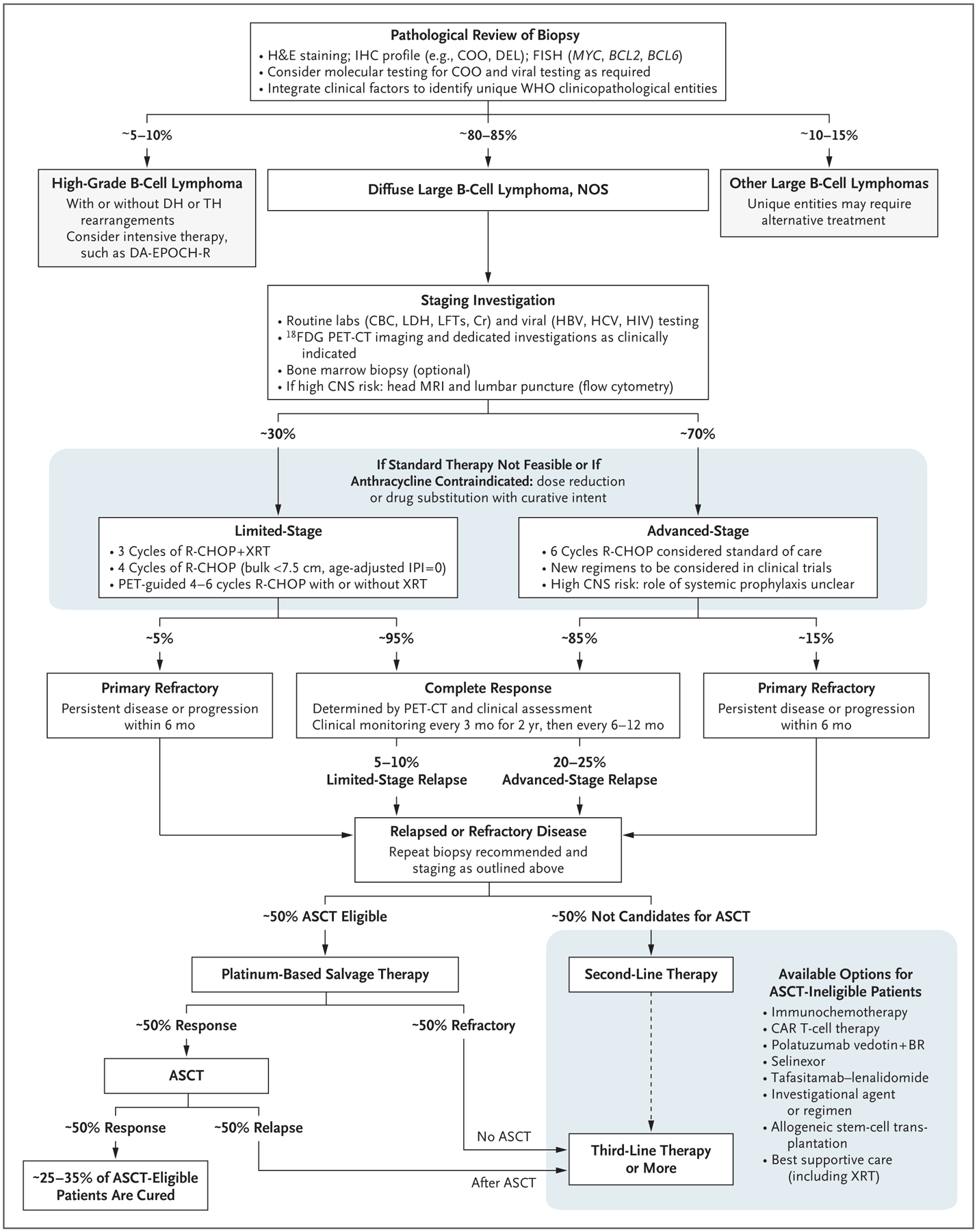
Large B-cell lymphomas, with an estimated 150,000 new cases annually worldwide, represent almost 30% of all cases of non-Hodgkin’s lymphoma. Patients typically present with progressive lymphadenopathy, extranodal disease, or both and require therapy. Despite the advanced stage at presentation in the majority of patients, more than 60% can be cured with R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone) immunochemotherapy (Fig. 1A). Patients with treatment failure after R-CHOP often have a poor outcome — in particular, those with disease that is refractory to frontline or subsequent therapies — although some patients can have a durable remission and be cured after secondary therapies. Over the past two decades, improved insights into large B-cell lymphomas, in terms of epidemiology, prognostic factors, and biologic heterogeneity, have led to a refinement of disease classification and the development of new therapeutic approaches.
Figures
Comment in
-
Diffuse Large B-Cell Lymphoma.N Engl J Med. 2021 Jun 10;384(23):2261-2262. doi: 10.1056/NEJMc2105452. N Engl J Med. 2021. PMID: 34107188 No abstract available.
References
-
- Rosenwald A, Wright G, Chan WC, et al. The use of molecular profiling to predict survival after chemotherapy for diffuse large-B-cell lymphoma. N Engl J Med 2002; 346: 1937–47. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous