

Elevated cerebrospinal fluid cytokine levels in tuberculous meningitis predict survival in response to dexamethasone
- PMID: 33658385
- PMCID: PMC7958233
- DOI: 10.1073/pnas.2024852118
Elevated cerebrospinal fluid cytokine levels in tuberculous meningitis predict survival in response to dexamethasone
Erratum in
-
Correction for Whitworth et al., Elevated cerebrospinal fluid cytokine levels in tuberculous meningitis predict survival in response to dexamethasone.Proc Natl Acad Sci U S A. 2021 Oct 12;118(41):e2116316118. doi: 10.1073/pnas.2116316118. Proc Natl Acad Sci U S A. 2021. PMID: 34607966 Free PMC article. No abstract available.
Abstract
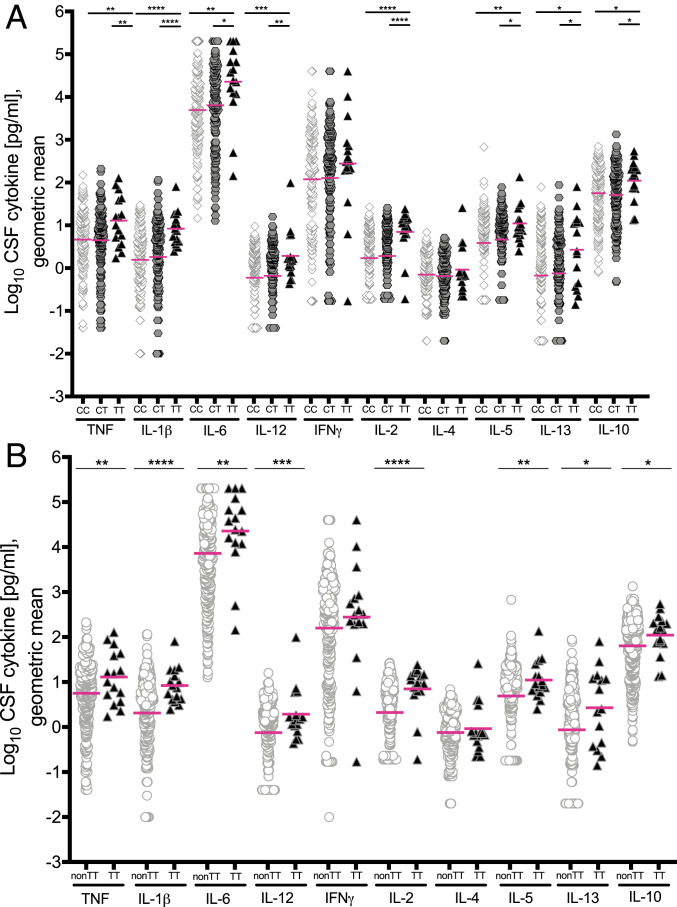
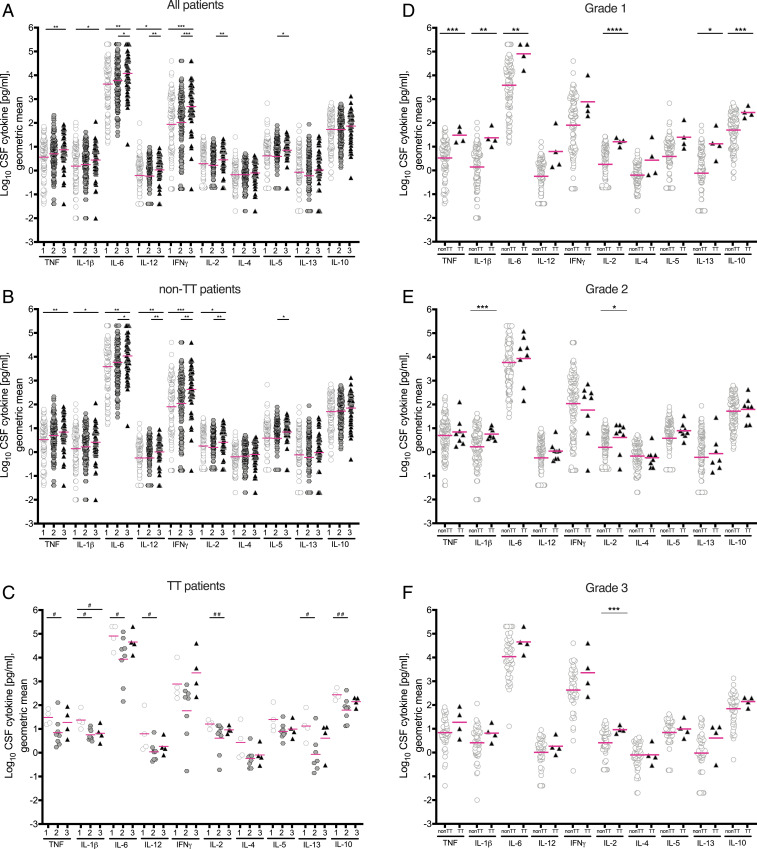
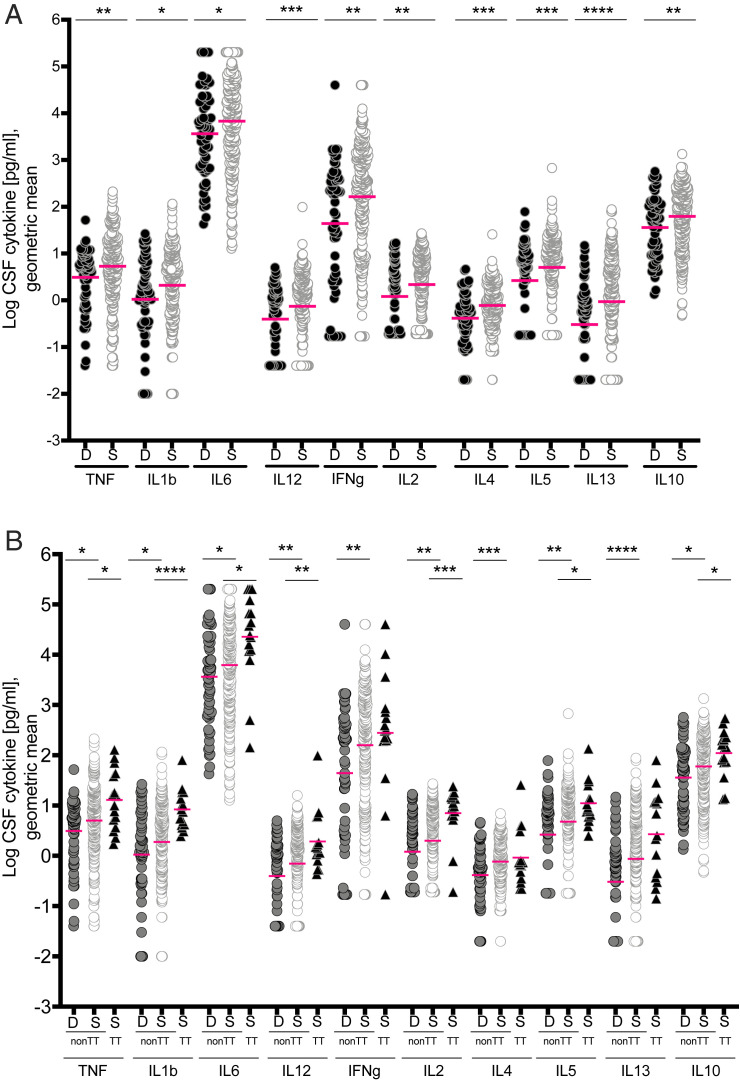
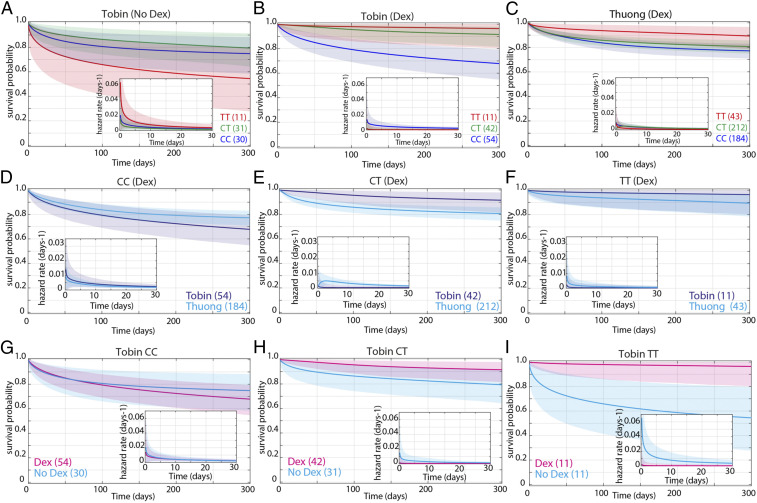
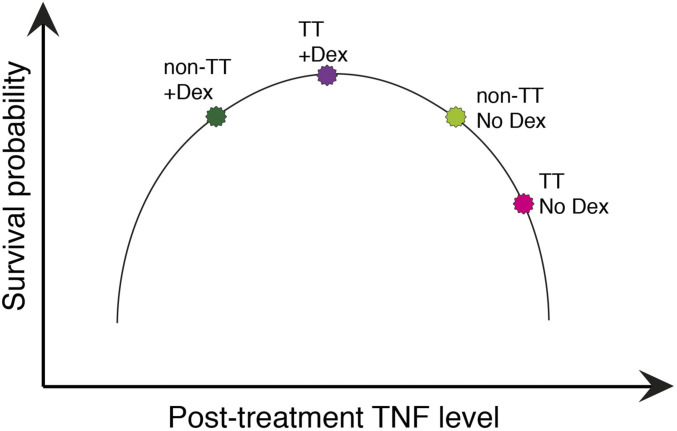
Adjunctive treatment with antiinflammatory corticosteroids like dexamethasone increases survival in tuberculosis meningitis. Dexamethasone responsiveness associates with a C/T variant in Leukotriene A4 Hydrolase (LTA4H), which regulates expression of the proinflammatory mediator leukotriene B4 (LTB4). TT homozygotes, with increased expression of LTA4H, have the highest survival when treated with dexamethasone and the lowest survival without. While the T allele is present in only a minority of the world's population, corticosteroids confer modest survival benefit worldwide. Using Bayesian methods, we examined how pretreatment levels of cerebrospinal fluid proinflammatory cytokines affect survival in dexamethasone-treated tuberculous meningitis. LTA4H TT homozygosity was associated with global cytokine increases, including tumor necrosis factor. Association between higher cytokine levels and survival extended to non-TT patients, suggesting that other genetic variants may also induce dexamethasone-responsive pathological inflammation. These findings warrant studies that tailor dexamethasone therapy to pretreatment cerebrospinal fluid cytokine concentrations, while searching for additional genetic loci shaping the inflammatory milieu.
Keywords: Bayesian analysis; corticosteroids; cytokines; inflammation; tuberculous meningitis.
Copyright © 2021 the Author(s). Published by PNAS.
Conflict of interest statement
Competing interest statement: D.M.T. and E.S. are coauthors on a 2018 meeting report.
Figures
References
-
- van Laarhoven A., et al., Clinical parameters, routine inflammatory markers, and LTA4H genotype as predictors of mortality among 608 patients with tuberculous meningitis in Indonesia. J. Infect. Dis. 215, 1029–1039 (2017). - PubMed
-
- Schoeman J. F., Elshof J. W., Laubscher J. A., Janse van Rensburg A., Donald P. R., The effect of adjuvant steroid treatment on serial cerebrospinal fluid changes in tuberculous meningitis. Ann. Trop. Paediatr. 21, 299–305 (2001). - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
