

HMGB1, anti-HMGB1 antibodies, and ratio of HMGB1/anti-HMGB1 antibodies as diagnosis indicator in fever of unknown origin
- PMID: 33658546
- PMCID: PMC7930274
- DOI: 10.1038/s41598-021-84477-2
HMGB1, anti-HMGB1 antibodies, and ratio of HMGB1/anti-HMGB1 antibodies as diagnosis indicator in fever of unknown origin
Abstract
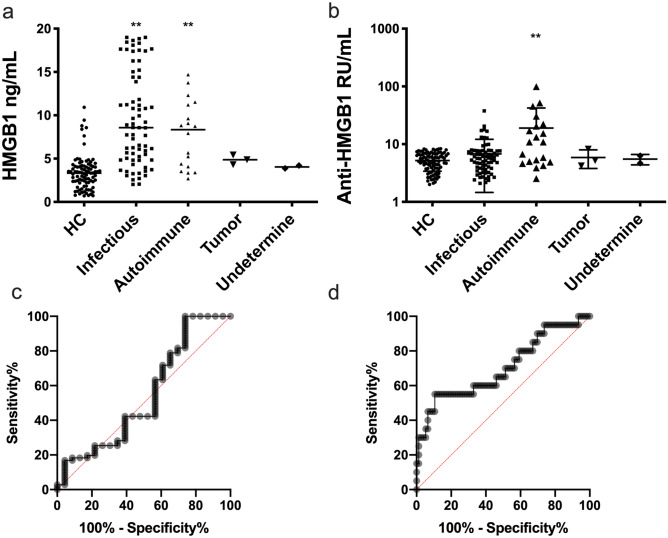
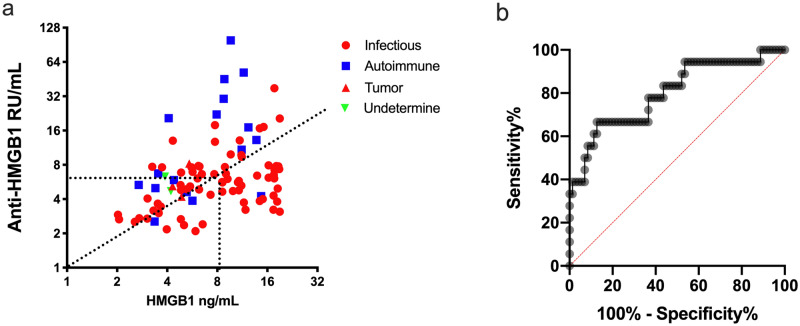
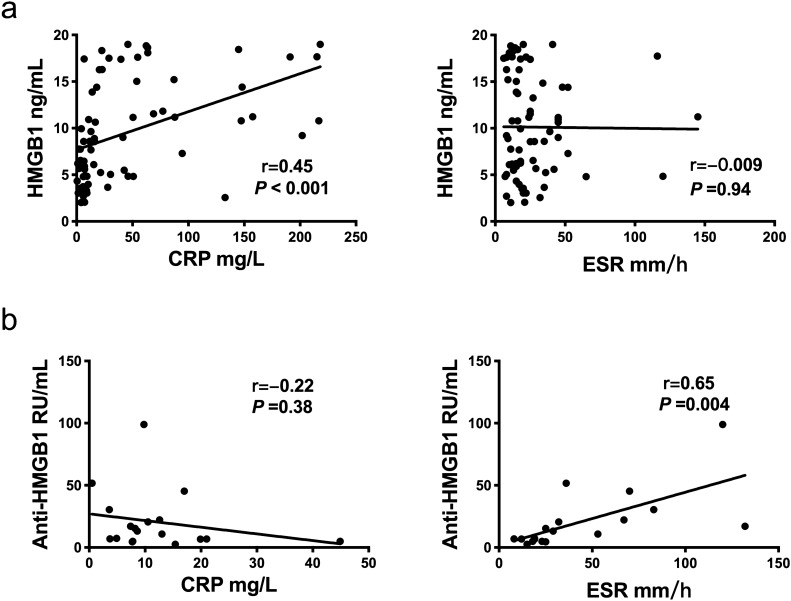
To evaluate the feasibility of serum HMGB1, anti-HMGB1 antibodies, and HMGB1/anti-HMGB1 ratio as a diagnosis indicator of initial clinical classification in patients with fever of unknown origin (FUO). Ninety-four patients with classical FUO and ninety healthy controls were enrolled in this study. The subjects' clinical data and serum were collected. The serum concentration of HMGB1 was detected by a commercial HMGB1 ELISA kit, while the serum concentration of anti-HMGB1 antibodies were detected by an in-house built anti-HMGB1 antibodies ELISA kit and further confirmed by immunoblotting. According to the hospital diagnosis on discharge, ninety-four FUO patients were divided into four groups, Infectious disease subgroup, autoimmune disease subgroup, malignant tumor subgroup, and undetermined subgroup. The concentrations of HMGB1 in the infectious disease subgroup and autoimmune disease subgroup were higher than those in the malignant tumor subgroup, undetermined subgroup, and healthy control group. The concentration of anti-HMGB1 antibodies in autoimmune disease subtype group was higher than those in other subgroups as well as healthy control group. According to the distribution of HMGB1 and anti-HMGB1 in scatter plots of the patients with FUO, we found that the ratio of serum HMGB1/anti-HMGB1 is an ideal clinical indicator for differential diagnosis of different subtypes of FUO. The best cut-off was 0.75, and the sensitivity, specificity, and AUC were 66.67%, 87.32%, and 0.8, respectively. Correlation analysis showed that serum concentration of HMGB1 was moderately correlated with CRP in infectious diseases subgroup, and the serum concentration of anti-HMGB1 antibodies was strongly correlated with erythrocyte sedimentation rate in autoimmune disease subgroup. Our study had showed that serum HMGB1/anti-HMGB1 antibodies ratio can help clinicians identify FUO subtypes, thereby avoiding many unnecessary examinations and tests, and improving the effectiveness of clinical diagnosis and treatment of FUO.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Fever of unknown origin: Clinical significance of the etiology and common inflammatory parameters.Diagn Microbiol Infect Dis. 2025 Jul;112(3):116801. doi: 10.1016/j.diagmicrobio.2025.116801. Epub 2025 Mar 12. Diagn Microbiol Infect Dis. 2025. PMID: 40120295
-
[Value of combined measurement of C-reactive protein, erythrocyte sedimentation rate, lactate dehydrogenase and serum ferritin in etiological diagnosis of fever of unknown origin in children].Zhongguo Dang Dai Er Ke Za Zhi. 2015 Sep;17(9):950-5. Zhongguo Dang Dai Er Ke Za Zhi. 2015. PMID: 26412177 Chinese.
-
Relationships between Causes of Fever of Unknown Origin and Inflammatory Markers: A Multicenter Collaborative Retrospective Study.Intern Med. 2015;54(16):1989-94. doi: 10.2169/internalmedicine.54.3313. Epub 2015 Aug 15. Intern Med. 2015. PMID: 26278289
-
Fever in Children and Fever of Unknown Origin.Indian J Pediatr. 2016 Jan;83(1):38-43. doi: 10.1007/s12098-015-1724-4. Epub 2015 Mar 1. Indian J Pediatr. 2016. PMID: 25724501 Review.
-
The management and the diagnosis of fever of unknown origin.Expert Rev Anti Infect Ther. 2013 Aug;11(8):805-15. doi: 10.1586/14787210.2013.814436. Expert Rev Anti Infect Ther. 2013. PMID: 23977936 Review.
Cited by
-
Biliary HMGB1 levels and biochemical indices in the assessment of acute obstructive septic cholangitis combined with septic shock.Clinics (Sao Paulo). 2025 Mar 6;80:100611. doi: 10.1016/j.clinsp.2025.100611. eCollection 2025. Clinics (Sao Paulo). 2025. PMID: 40054422 Free PMC article.
-
Small RNA and Toll-like receptor interactions: origins and disease mechanisms.Trends Biochem Sci. 2025 May;50(5):385-401. doi: 10.1016/j.tibs.2025.01.004. Epub 2025 Feb 15. Trends Biochem Sci. 2025. PMID: 39956743 Review.
-
Association between high-mobility group box 1 levels and febrile seizures in children: a systematic review and meta-analysis.Sci Rep. 2023 Mar 3;13(1):3619. doi: 10.1038/s41598-023-30713-w. Sci Rep. 2023. PMID: 36869074 Free PMC article.
-
Anti-Oxidized Low-Density Lipoprotein Antibodies Before and After Intravenous Immunoglobulin Therapy in Kawasaki Disease - Evidence for a Potentially Protective Role.Circ Rep. 2025 Apr 16;7(5):359-364. doi: 10.1253/circrep.CR-25-0018. eCollection 2025 May 9. Circ Rep. 2025. PMID: 40352122 Free PMC article.
References
-
- Attard L, Tadolini M, De Rose DU, Cattalini M. Overview of fever of unknown origin in adult and paediatric patients. Clin. Exp. Rheumatol. 2018;36(Suppl 110):10–24. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
