

Brain injury after 50 h of lung-protective mechanical ventilation in a preclinical model
- PMID: 33658581
- PMCID: PMC7930247
- DOI: 10.1038/s41598-021-84440-1
Brain injury after 50 h of lung-protective mechanical ventilation in a preclinical model
Abstract
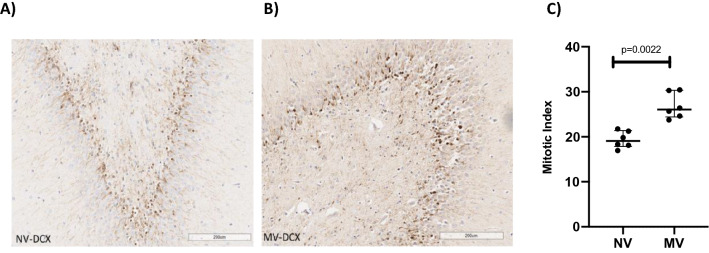
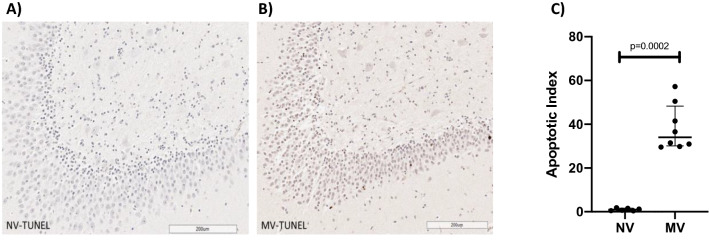
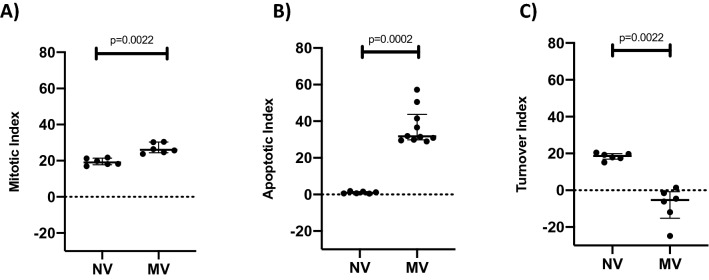
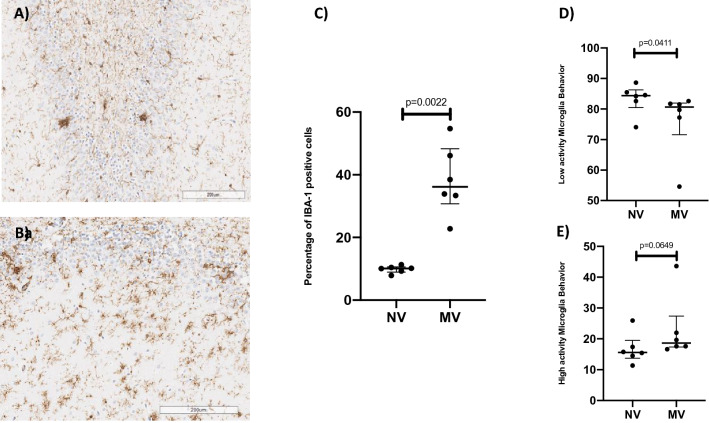
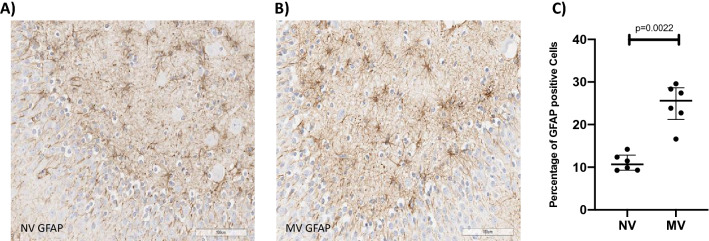
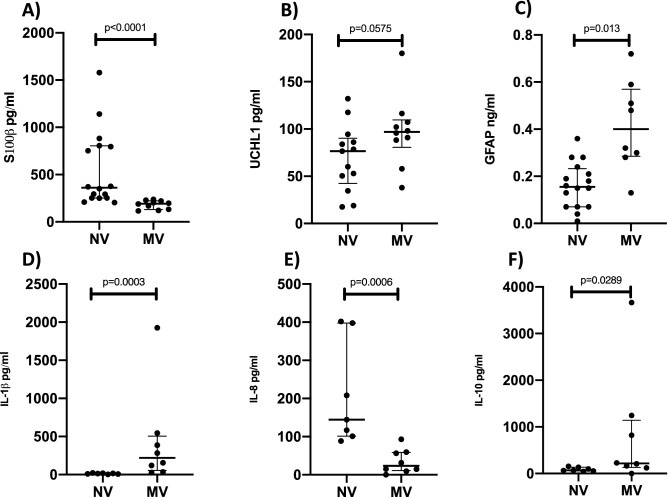
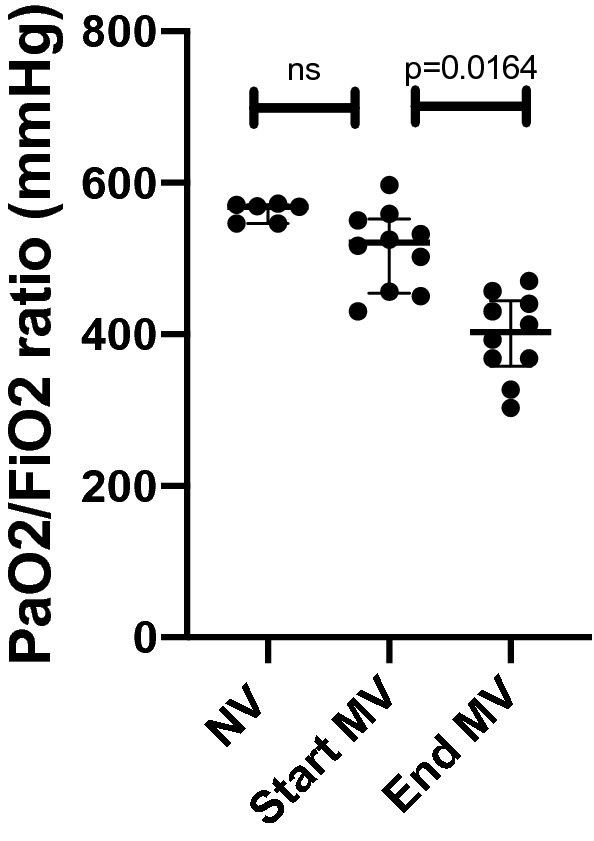
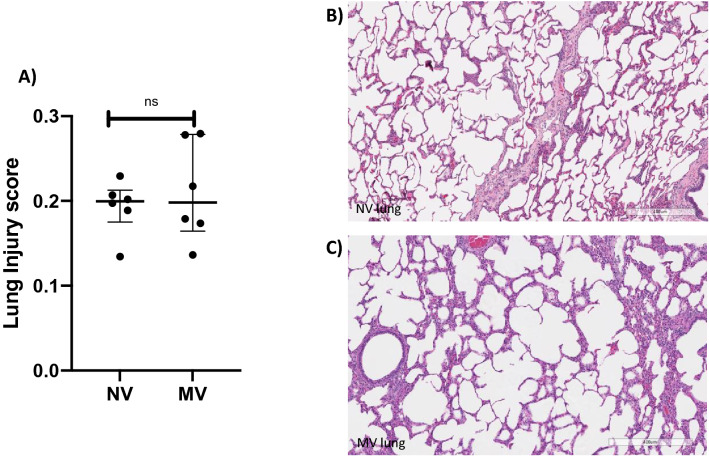
Mechanical ventilation is the cornerstone of the Intensive Care Unit. However, it has been associated with many negative consequences. Recently, ventilator-induced brain injury has been reported in rodents under injurious ventilation settings. Our group wanted to explore the extent of brain injury after 50 h of mechanical ventilation, sedation and physical immobility, quantifying hippocampal apoptosis and inflammation, in a normal-lung porcine study. After 50 h of lung-protective mechanical ventilation, sedation and immobility, greater levels of hippocampal apoptosis and neuroinflammation were clearly observed in the mechanically ventilated group, in comparison to a never-ventilated group. Markers in the serum for astrocyte damage and neuronal damage were also higher in the mechanically ventilated group. Therefore, our study demonstrated that considerable hippocampal insult can be observed after 50 h of lung-protective mechanical ventilation, sedation and physical immobility.
Conflict of interest statement
E.C.R, K.C.F, M.O, M.N and S.C.R have received consulting fees from Lungpacer Medical, Inc. T.G.B, D.E and M.G are employees of Lungpacer Medical, Inc. S.C.R is listed on a patent for Lungpacer Medical, Inc.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
