

Stillbirths, Neonatal Morbidity, and Mortality in Health-Facility Deliveries in Urban Gambia
- PMID: 33659227
- PMCID: PMC7917219
- DOI: 10.3389/fped.2021.579922
Stillbirths, Neonatal Morbidity, and Mortality in Health-Facility Deliveries in Urban Gambia
Abstract
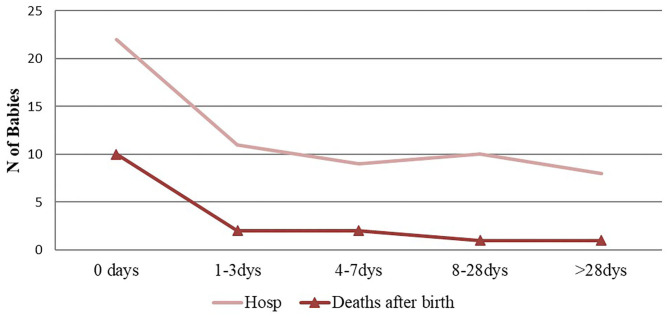
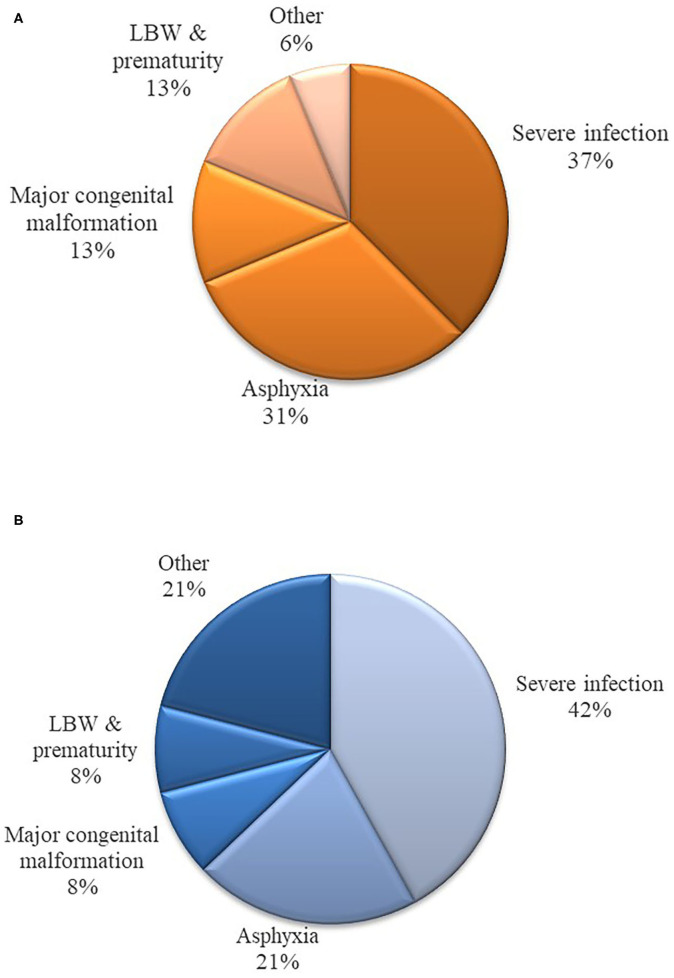
Background: The Gambia Demographic and Health Survey 2013 data showed that up to 63% of deliveries in the country occur in health facilities. Despite such a high rate, there are few facility-based studies on delivery outcomes in the country. This analysis ancillary to a randomized control trial describes occurrence of poor pregnancy outcomes in a cohort of women and their infants delivering in a government health facility in urban Gambia. Methods: Using clinical information obtained during the trial, we calculated rates of poor pregnancy outcomes including stillbirths, hospitalization and neonatal deaths. Logistic regression was used to calculate odds ratio (OR) and 95% confidence interval (CI) in the risk factors analysis. Results: Between April 2013 and 2014, 829 mothers delivered 843 babies, including 13 stillbirths [15.4 (7.1-23.8)] per 1,000 births. Among 830 live born infants, 7.6% (n = 63) required hospitalization during the 8-week follow-up period. Most of these hospitalizations (74.6%) occurred during the early neonatal period (<7 days of life). Severe clinical infections (i.e., sepsis, meningitis and pneumonia) (n = 27) were the most common diagnoses, followed by birth asphyxia (n = 13), major congenital malformations (n = 10), jaundice (n = 6) and low birth weight (n = 5). There were sixteen neonatal deaths, most of which also occurred during the early neonatal period. Overall, neonatal mortality rate (NMR) and perinatal mortality rate (PMR) were 19.3 (CI: 9.9-28.7) per 1,000 live births and 26.1 (CI: 15.3-36.9) per 1,000 total births, respectively. Severe clinical infections and birth asphyxia accounted for 37 and 31% of neonatal deaths, respectively. The risk of hospitalization was higher among neonates with severe congenital malformations, low birth weight, twin deliveries, and those born by cesarean section. Risk of mortality was higher among neonates with severe congenital malformations and twin deliveries. Conclusion: Neonatal hospitalization and deaths in our cohort were high. Although vertical interventions may reduce specific causes of morbidity and mortality, data indicate the need for a holistic approach to significantly improve the rates of poor pregnancy outcomes. Critically, a focus on decreasing the high rate of stillbirths is warranted. Clinical Trial Registration: ClinicalTrials.gov Identifier: NCT01800942.
Keywords: The Gambia; birth asphyxia; congenital malformation; hospitalization; neonatal mortality; sepsis; stillbirth.
Copyright © 2021 Camara, Oluwalana, Miyahara, Lush, Kampmann, Manneh, Okomo, D'Alessandro and Roca.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Blencowe H, Vos T, Lee AC, Philips R, Lozano R, Alvarado MR, et al. . Estimates of neonatal morbidities and disabilities at regional and global levels for 2010: introduction, methods overview, and relevant findings from the Global Burden of Disease study. Pediatr Res. (2013) 74(Suppl. 1):4–16. 10.1038/pr.2013.203 - DOI - PMC - PubMed
-
- UN IGME Child Mortality Report 2018 . Report. New York, NY: United Nations; (2018).
-
- Abubakar II, Tillmann T, Banerjee A. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. (2015) 385:117–71. 10.1016/S0140-6736(14)61682-2 - DOI - PMC - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous