

The conduction velocity-potassium relationship in the heart is modulated by sodium and calcium
- PMID: 33660028
- PMCID: PMC7940307
- DOI: 10.1007/s00424-021-02537-y
The conduction velocity-potassium relationship in the heart is modulated by sodium and calcium
Abstract
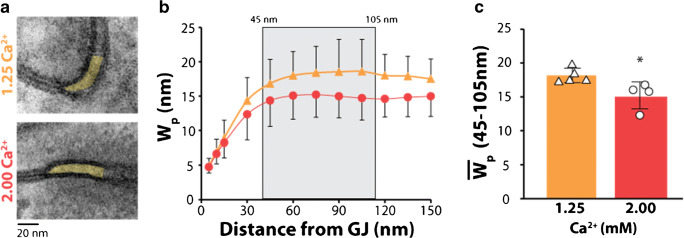
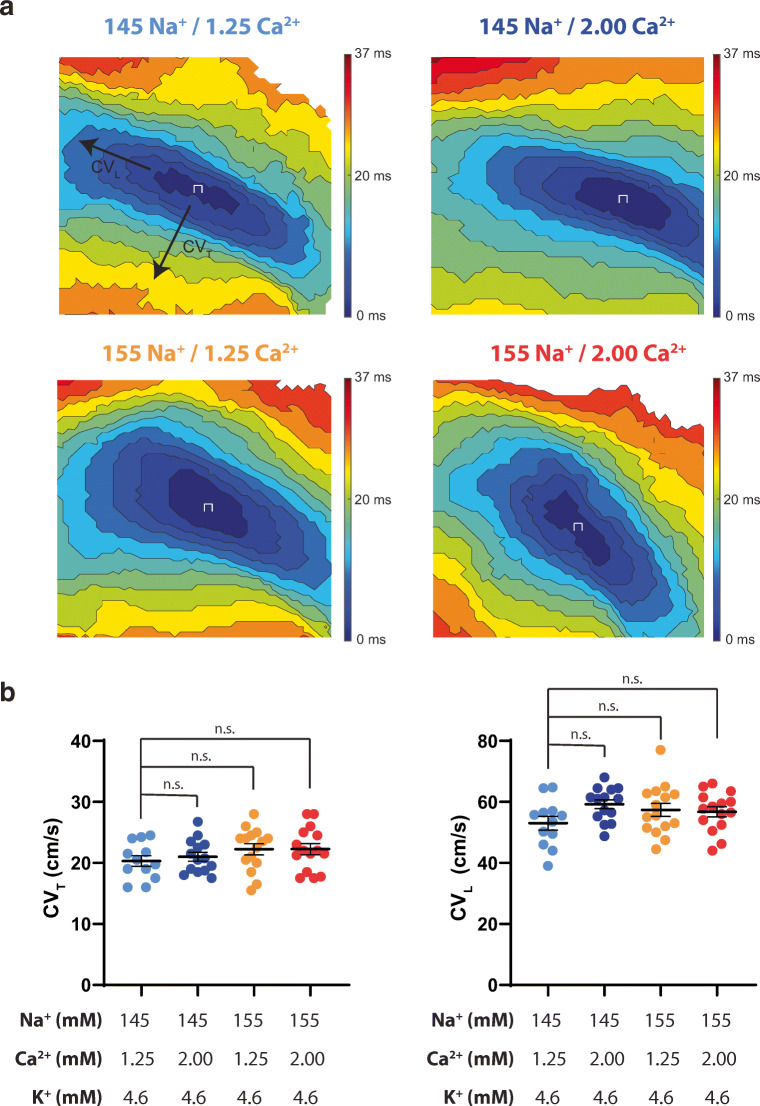
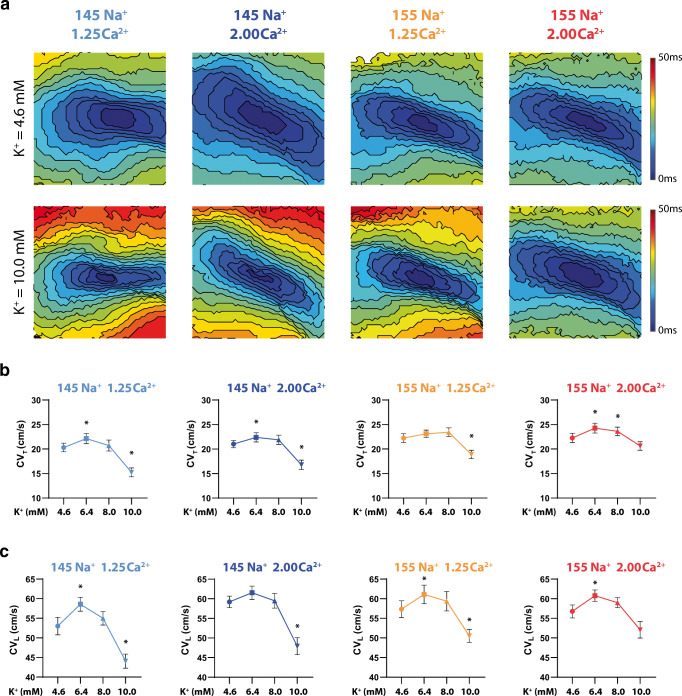
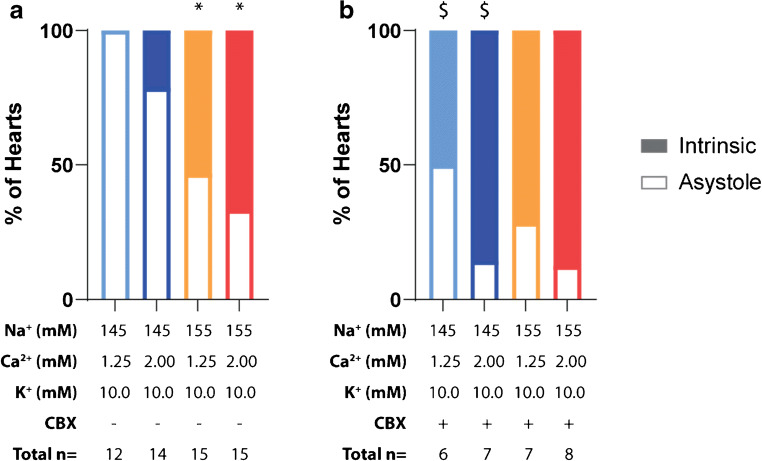
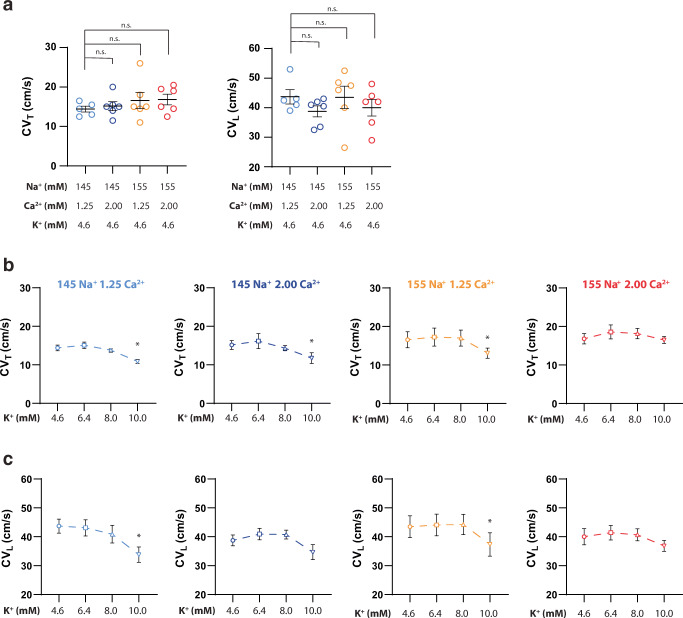
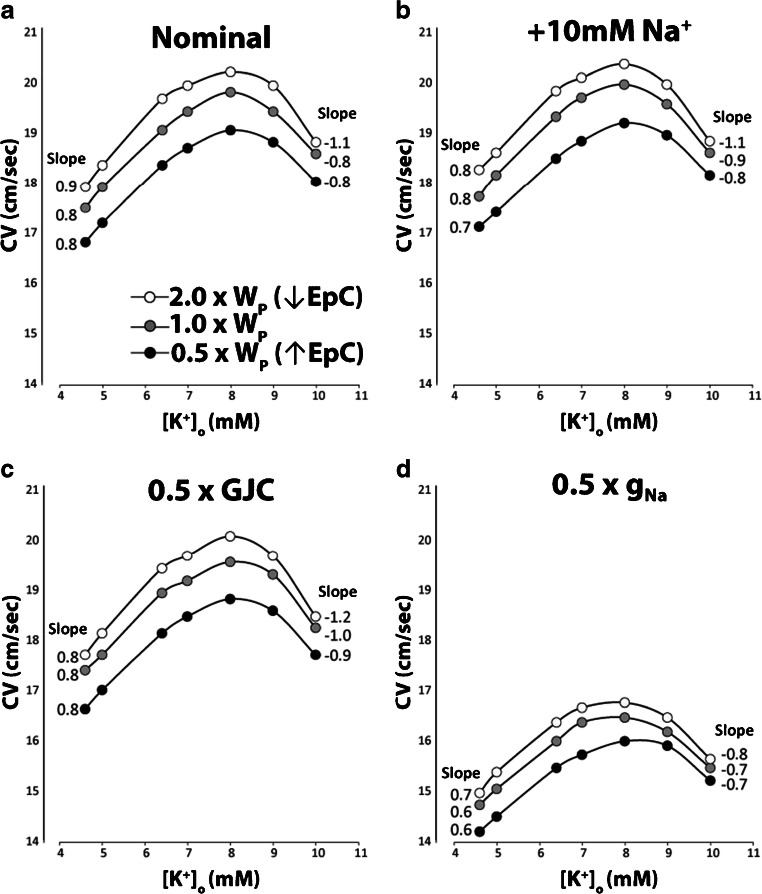
The relationship between cardiac conduction velocity (CV) and extracellular potassium (K+) is biphasic, with modest hyperkalemia increasing CV and severe hyperkalemia slowing CV. Recent studies from our group suggest that elevating extracellular sodium (Na+) and calcium (Ca2+) can enhance CV by an extracellular pathway parallel to gap junctional coupling (GJC) called ephaptic coupling that can occur in the gap junction adjacent perinexus. However, it remains unknown whether these same interventions modulate CV as a function of K+. We hypothesize that Na+, Ca2+, and GJC can attenuate conduction slowing consequent to severe hyperkalemia. Elevating Ca2+ from 1.25 to 2.00 mM significantly narrowed perinexal width measured by transmission electron microscopy. Optically mapped, Langendorff-perfused guinea pig hearts perfused with increasing K+ revealed the expected biphasic CV-K+ relationship during perfusion with different Na+ and Ca2+ concentrations. Neither elevating Na+ nor Ca2+ alone consistently modulated the positive slope of CV-K+ or conduction slowing at 10-mM K+; however, combined Na+ and Ca2+ elevation significantly mitigated conduction slowing at 10-mM K+. Pharmacologic GJC inhibition with 30-μM carbenoxolone slowed CV without changing the shape of CV-K+ curves. A computational model of CV predicted that elevating Na+ and narrowing clefts between myocytes, as occur with perinexal narrowing, reduces the positive and negative slopes of the CV-K+ relationship but do not support a primary role of GJC or sodium channel conductance. These data demonstrate that combinatorial effects of Na+ and Ca2+ differentially modulate conduction during hyperkalemia, and enhancing determinants of ephaptic coupling may attenuate conduction changes in a variety of physiologic conditions.
Keywords: Calcium; Cardiac Electrophysiology; Hyperkalemia; Langendorff; Sodium.
Figures
References
-
- Ashpole NM, Herren AW, Ginsburg KS, Brogan JD, Johnson DE, Cummins TR, Bers DM, Hudmon A. Ca 2+/calmodulin-dependent protein kinase II (CaMKII) regulates cardiac sodium channel Na V 1.5 gating by multiple phosphorylation sites. J Biol Chem. 2012;287(24):19856–19869. doi: 10.1074/jbc.M111.322537. - DOI - PMC - PubMed
-
- Bates D, Mächler M, Bolker B, Walker S (2015) Fitting linear mixed-effects models using lme4. J Stat Softw 67(1). 10.18637/jss.v067.i01
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
