

Bystander Cardiopulmonary Resuscitation Quality: Potential for Improvements in Cardiac Arrest Resuscitation
- PMID: 33660519
- PMCID: PMC8174211
- DOI: 10.1161/JAHA.120.017930
Bystander Cardiopulmonary Resuscitation Quality: Potential for Improvements in Cardiac Arrest Resuscitation
Abstract
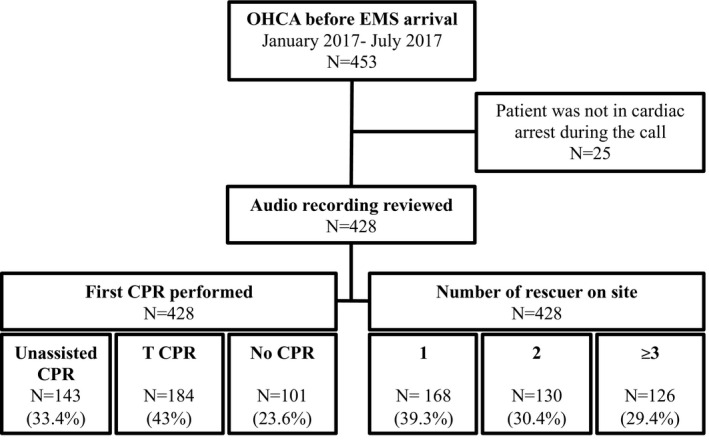
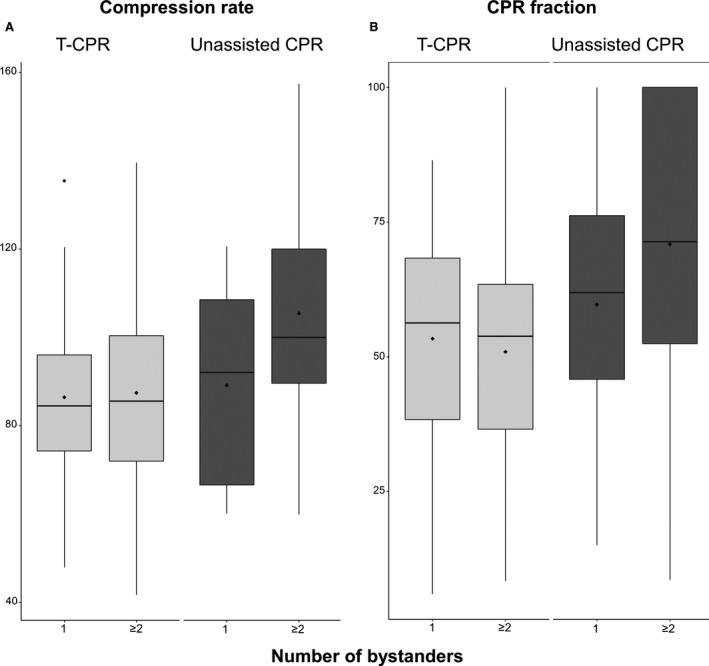
Background Bystander cardiopulmonary resuscitation (CPR) is a critical intervention to improve survival following out-of-hospital cardiac arrest. We evaluated the quality of bystander CPR and whether performance varied according to the number of bystanders or provision of telecommunicator CPR (TCPR). Methods and Results We investigated non-traumatic out-of-hospital cardiac arrest occurring in a large metropolitan emergency medical system during a 6-month period. Information about bystander care was ascertained through review of the 9-1-1 recordings in addition to emergency medical system and hospital records to determine bystander CPR status (none versus TCPR versus unassisted), the number of bystanders on-scene, and CPR performance metrics of compression fraction and compression rate. Of the 428 eligible out-of-hospital cardiac arrest, 76.4% received bystander CPR including 43.7% unassisted CPR and 56.3% TCPR; 35.2% had one bystander, 33.3% had 2 bystanders, and 31.5% had ≥3 bystanders. Overall compression fraction was 59% with a compression rate of 88 per minute. CPR differed according to TCPR status (fraction=52%, rate=87 per minute for TCPR versus fraction=69%, rate=102 for unassisted CPR, P<0.05 for each comparison) and the number of bystanders (fraction=55%, rate=87 per minute for 1 bystander, fraction=59%, rate=89 for 2 bystanders, fraction=65%, rate=97 for ≥3 bystanders, test for trend P<0.05 for each metric). Additional bystander actions were uncommon to include rotation of compressors (3.1%) or application of an automated external defibrillator (8.0%). Conclusions Bystander CPR quality as gauged by compression fraction and rate approached guideline goals though performance depended upon the type of CPR and number of bystanders.
Keywords: dispatch‐assisted cardiopulmonary resuscitation; out of hospital cardiac arrest; quality in health care; telecommunicator cardiopulmonary resuscitation.
Conflict of interest statement
None.
Figures
Similar articles
-
Community-Wide Dissemination of Bystander Cardiopulmonary Resuscitation and Automated External Defibrillator Use Using a 45-Minute Chest Compression-Only Cardiopulmonary Resuscitation Training.J Am Heart Assoc. 2019 Jan 8;8(1):e009436. doi: 10.1161/JAHA.118.009436. J Am Heart Assoc. 2019. PMID: 30612478 Free PMC article.
-
Analysis of bystander CPR quality during out-of-hospital cardiac arrest using data derived from automated external defibrillators.Resuscitation. 2018 Jul;128:138-143. doi: 10.1016/j.resuscitation.2018.05.012. Epub 2018 May 16. Resuscitation. 2018. PMID: 29753856
-
Quality of bystander cardiopulmonary resuscitation during real-life out-of-hospital cardiac arrest.Resuscitation. 2017 Nov;120:63-70. doi: 10.1016/j.resuscitation.2017.09.006. Epub 2017 Sep 10. Resuscitation. 2017. PMID: 28903056
-
Impact of dispatcher-assisted cardiopulmonary resuscitation on neurologically intact survival in out-of-hospital cardiac arrest: a systematic review.Scand J Trauma Resusc Emerg Med. 2021 May 24;29(1):70. doi: 10.1186/s13049-021-00875-5. Scand J Trauma Resusc Emerg Med. 2021. PMID: 34030706 Free PMC article.
-
Improving bystander cardiopulmonary resuscitation.Curr Opin Crit Care. 2011 Jun;17(3):219-24. doi: 10.1097/MCC.0b013e32834697d8. Curr Opin Crit Care. 2011. PMID: 21499092 Review.
Cited by
-
Enhancing Bystander Intervention: Insights from the Utstein Analysis of Out-of-Hospital Cardiac Arrests in Slovenia.Medicina (Kaunas). 2024 Jul 29;60(8):1227. doi: 10.3390/medicina60081227. Medicina (Kaunas). 2024. PMID: 39202509 Free PMC article.
-
Sudden cardiac arrest prediction via deep learning electrocardiogram analysis.Eur Heart J Digit Health. 2025 Feb 25;6(2):170-179. doi: 10.1093/ehjdh/ztae088. eCollection 2025 Mar. Eur Heart J Digit Health. 2025. PMID: 40110219 Free PMC article.
-
Drones for Saving Life: Reimagining War Technology.Circ Cardiovasc Qual Outcomes. 2024 Apr;17(4):e010908. doi: 10.1161/CIRCOUTCOMES.124.010908. Epub 2024 Mar 26. Circ Cardiovasc Qual Outcomes. 2024. PMID: 38529633 Free PMC article. No abstract available.
-
Effectiveness of school-based CPR training among adolescents to enhance knowledge and skills in CPR: A systematic review.Curationis. 2022 Nov 18;45(1):e1-e9. doi: 10.4102/curationis.v45i1.2325. Curationis. 2022. PMID: 36453813 Free PMC article.
-
Association between bystander physical limitations, delays in chest compression during telecommunicator-assisted cardiopulmonary resuscitation, and outcome after out-of-hospital cardiac arrest.Resuscitation. 2023 Jul;188:109816. doi: 10.1016/j.resuscitation.2023.109816. Epub 2023 May 3. Resuscitation. 2023. PMID: 37146672 Free PMC article.
References
-
- Benjamin EJ, Muntner P, Alonso A, Bittencourt MS, Callaway CW, Carson AP, Chamberlain AM, Chang AR, Cheng S, Das SR, et al. Heart disease and stroke statistics—2019 update: a report from the American Heart Association. Circulation. 2019;139:e56–e528. DOI: 10.1161/CIR.0000000000000659. - DOI - PubMed
-
- Nakashima T, Noguchi T, Tahara Y, Nishimura K, Yasuda S, Onozuka D, Iwami T, Yonemoto N, Nagao K, Nonogi H, et al. Public‐access defibrillation and neurological outcomes in patients with out‐of‐hospital cardiac arrest in Japan: a population‐based cohort study. Lancet. 2020;394:2255–2262. DOI: 10.1016/S0140-6736(19)32488-2. - DOI - PubMed
-
- Kobayashi D, Kitamura T, Kiyohara K, Nishiyama C, Hayashida S, Matsuyama T, Katayama Y, Shimamoto T, Kiguchi T, Okabayashi S, et al. Cardiopulmonary resuscitation performed by off‐duty medical professionals versus laypersons and survival from out‐of‐hospital cardiac arrest among adult patients. Resuscitation. 2019;135:66–72. DOI: 10.1016/j.resuscitation.2019.01.005. - DOI - PubMed
-
- Derkenne C, Jost D, Thabouillot O, Briche F, Travers S, Frattini B, Lesaffre X, Kedzierewicz R, Roquet F, de Charry F, et al. Improving emergency call detection of Out‐of‐Hospital Cardiac Arrests in the Greater Paris area: efficiency of a global system with a new method of detection. Resuscitation. 2020;146:34–42. DOI: 10.1016/j.resuscitation.2019.10.038. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
