

Development and validation of a predictive model of in-hospital mortality in COVID-19 patients
- PMID: 33661939
- PMCID: PMC7932507
- DOI: 10.1371/journal.pone.0247676
Development and validation of a predictive model of in-hospital mortality in COVID-19 patients
Abstract
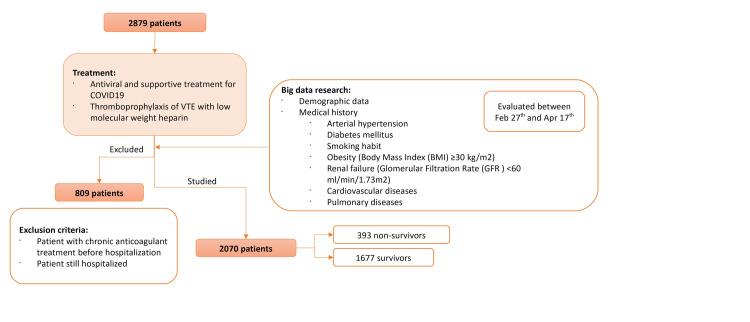
We retrospectively evaluated 2879 hospitalized COVID-19 patients from four hospitals to evaluate the ability of demographic data, medical history, and on-admission laboratory parameters to predict in-hospital mortality. Association of previously published risk factors (age, gender, arterial hypertension, diabetes mellitus, smoking habit, obesity, renal failure, cardiovascular/ pulmonary diseases, serum ferritin, lymphocyte count, APTT, PT, fibrinogen, D-dimer, and platelet count) with death was tested by a multivariate logistic regression, and a predictive model was created, with further validation in an independent sample. A total of 2070 hospitalized COVID-19 patients were finally included in the multivariable analysis. Age 61-70 years (p<0.001; OR: 7.69; 95%CI: 2.93 to 20.14), age 71-80 years (p<0.001; OR: 14.99; 95%CI: 5.88 to 38.22), age >80 years (p<0.001; OR: 36.78; 95%CI: 14.42 to 93.85), male gender (p<0.001; OR: 1.84; 95%CI: 1.31 to 2.58), D-dimer levels >2 ULN (p = 0.003; OR: 1.79; 95%CI: 1.22 to 2.62), and prolonged PT (p<0.001; OR: 2.18; 95%CI: 1.49 to 3.18) were independently associated with increased in-hospital mortality. A predictive model performed with these parameters showed an AUC of 0.81 in the development cohort (n = 1270) [sensitivity of 95.83%, specificity of 41.46%, negative predictive value of 98.01%, and positive predictive value of 24.85%]. These results were then validated in an independent data sample (n = 800). Our predictive model of in-hospital mortality of COVID-19 patients has been developed, calibrated and validated. The model (MRS-COVID) included age, male gender, and on-admission coagulopathy markers as positively correlated factors with fatal outcome.
Conflict of interest statement
All the authors are employees of Quironsalud. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
